Phenotypic Characteristics and Development of a Hospitalization Prediction Risk Score for Outpatients with Diabetes and COVID-19: The DIABCOVID Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Data Collection
2.3. Aim of the Study
2.4. Endpoints
2.5. Statistical Analysis
2.5.1. Development of a Risk–Score Model
2.5.2. External Validation of the Risk–Score Model
3. Results
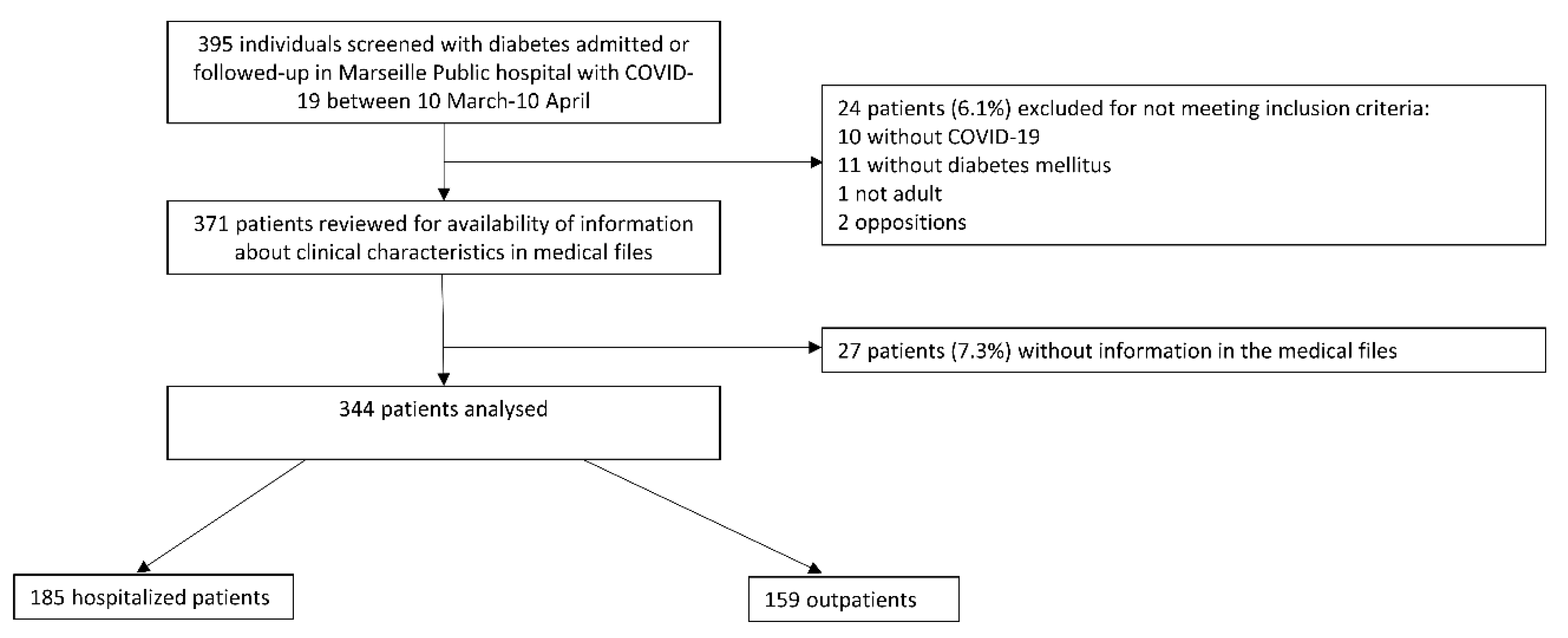
3.1. Population
3.2. Differences in Demographic and Diabetes-Related Characteristics between Hospitalized and Outpatients
3.3. Characteristics of COVID-19 during First Examination, and Differences between In- and Outpatients
3.4. Predictive Criteria for Hospitalization and Model Development of an Easy-to-Use Pragmatic Score for Clinicians
3.5. Secondary Endpoints
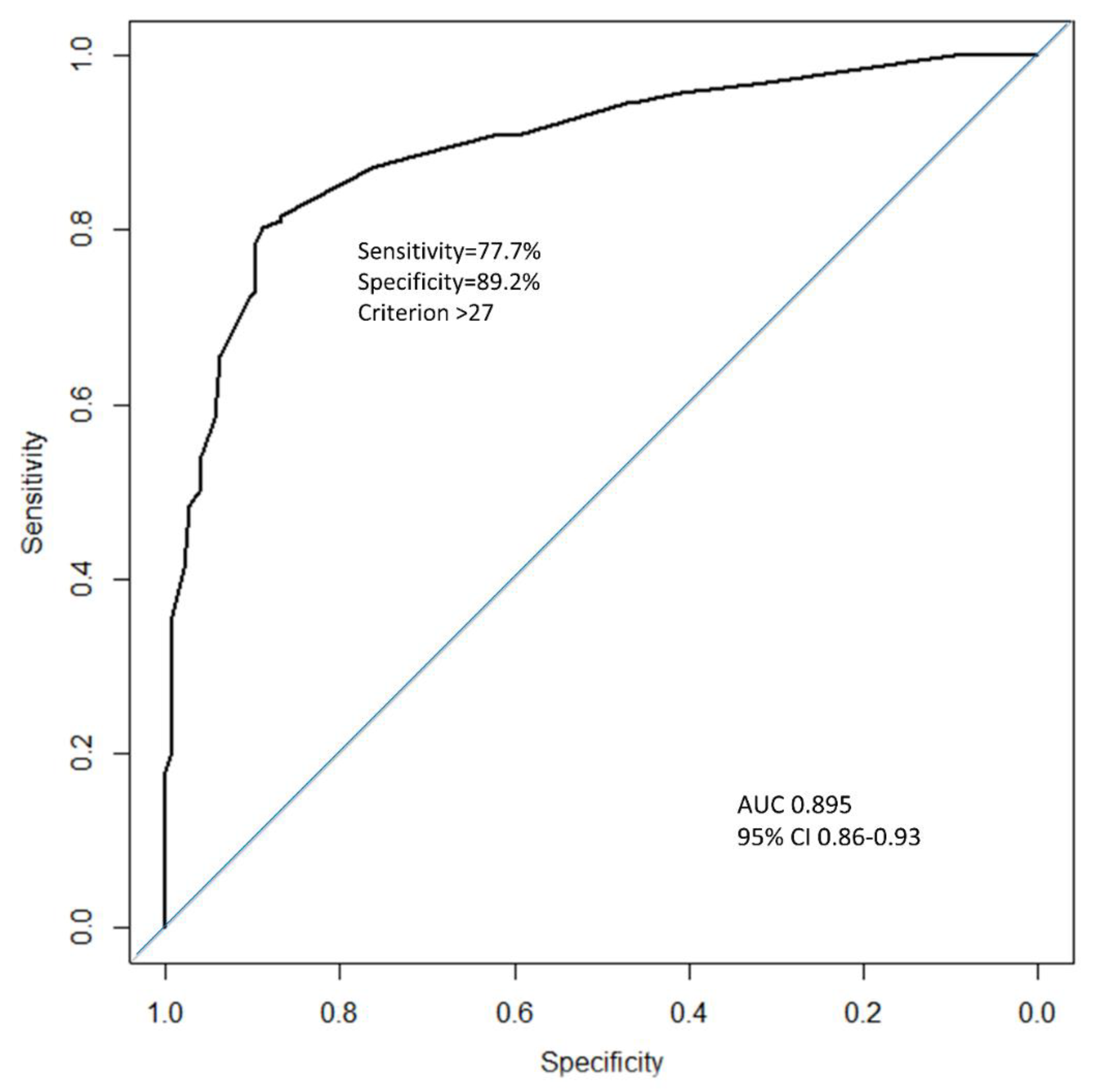
3.6. External Validation of the Diabscore in Two Other Cohorts
3.6.1. External Validation of the Diabscore in Another Period of Time
3.6.2. External Validation of the Diabscore in the Whole CORONADO Cohort
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, 81, e16–e25. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020. [Google Scholar] [CrossRef]
- Huang, I.; Lim, M.A.; Pranata, R. Diabetes mellitus is associated with increased mortality and severity of disease in COVID-19 pneumonia—A systematic review, meta-analysis, and meta-regression. Diabetes Metab. Syndr. 2020, 14, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Muniyappa, R.; Gubbi, S. COVID-19 pandemic, coronaviruses, and diabetes mellitus. Am. J. Physiol. Endocrinol. Metab. 2020, 318, E736–E741. [Google Scholar] [CrossRef] [Green Version]
- Rello, J.; Storti, E.; Belliato, M.; Serrano, R. Clinical phenotypes of SARS-CoV-2: Implications for clinicians and researchers. Eur. Respir. J. 2020, 55. [Google Scholar] [CrossRef]
- Wilkerson, R.G.; Adler, J.D.; Shah, N.G.; Brown, R. Silent hypoxia: A harbinger of clinical deterioration in patients with COVID-19. Am. J. Emerg. Med. 2020. [Google Scholar] [CrossRef]
- Cariou, B.; Hadjadj, S.; Wargny, M.; Pichelin, M.; Al-Salameh, A.; Allix, I.; Amadou, C.; Arnault, G.; Baudoux, F.; Bauduceau, B.; et al. Phenotypic characteristics and prognosis of inpatients with COVID-19 and diabetes: The CORONADO study. Diabetologia 2020, 63, 1500–1515. [Google Scholar] [CrossRef]
- Nguyen, D.T.; Graviss, E.A. Development and validation of a prognostic score to predict tuberculosis mortality. J. Infect. 2018, 77, 283–290. [Google Scholar] [CrossRef] [Green Version]
- Logistf: Firth’s Bias-Reduced Logistic Regression Version 1.24 from CRAN. Available online: https://rdrr.io/cran/logistf/ (accessed on 21 September 2020).
- Shabto, J.M.; Loerinc, L.; O’Keefe, G.A.; O’Keefe, J. Characteristics and outcomes of COVID-19 positive patients with diabetes managed as outpatients. Diabetes Res. Clin. Pract. 2020, 164, 108229. [Google Scholar] [CrossRef]
- Rubino, F.; Amiel, S.A.; Zimmet, P.; Alberti, G.; Bornstein, S.; Eckel, R.H.; Mingrone, G.; Boehm, B.; Cooper, M.E.; Chai, Z.; et al. New-Onset Diabetes in Covid-19. N. Engl. J. Med. 2020, 383, 789–790. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; She, Z.-G.; Cheng, X.; Qin, J.-J.; Zhang, X.-J.; Cai, J.; Lei, F.; Wang, H.; Xie, J.; Wang, W.; et al. Association of Blood Glucose Control and Outcomes in Patients with COVID-19 and Pre-existing Type 2 Diabetes. Cell Metab. 2020, 31, 1068–1077.e3. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Guan, W.-J.; Liang, W.-H.; Zhao, Y.; Liang, H.-R.; Chen, Z.-S.; Li, Y.-M.; Liu, X.-Q.; Chen, R.-C.; Tang, C.-L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55. [Google Scholar] [CrossRef] [Green Version]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; The Northwell COVID-19 Research Consortium; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; et al. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020. [Google Scholar] [CrossRef]
- Davies, M.J.; D’Alessio, D.A.; Fradkin, J.; Kernan, W.N.; Mathieu, C.; Mingrone, G.; Rossing, P.; Tsapas, A.; Wexler, D.J.; Buse, J.B. Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2018, 41, 2669–2701. [Google Scholar] [CrossRef] [Green Version]
- Maddaloni, E.; D’Onofrio, L.; Alessandri, F.; Mignogna, C.; Leto, G.; Coraggio, L.; Sterpetti, S.; Pascarella, G.; Mezzaroma, I.; Lichtner, M.; et al. Clinical features of patients with type 2 diabetes with and without Covid-19: A case control study (CoViDiab I). Diabetes Res. Clin. Pract. 2020, 169, 108454. [Google Scholar] [CrossRef]
- Maddaloni, E.; D’Onofrio, L.; Alessandri, F.; Mignogna, C.; Leto, G.; Pascarella, G.; Mezzaroma, I.; Lichtner, M.; Pozzilli, P.; Agrò, F.E.; et al. Cardiometabolic multimorbidity is associated with a worse Covid-19 prognosis than individual cardiometabolic risk factors: A multicentre retrospective study (CoViDiab II). Cardiovasc. Diabetol. 2020, 19, 164. [Google Scholar] [CrossRef]
- Zhou, Y.; Chi, J.; Lv, W.; Wang, Y. Obesity and diabetes as high-risk factors for severe coronavirus disease 2019 (COVID-19). Diabetes Metab. Res. Rev. 2020. [Google Scholar] [CrossRef]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M.; et al. High Prevalence of Obesity in Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) Requiring Invasive Mechanical Ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Du, S.; Green, W.D.; Beck, M.A.; Algaith, T.; Herbst, C.H.; Alsukait, R.F.; Alluhidan, M.; Alazemi, N.; Shekar, M. Individuals with obesity and COVID-19: A global perspective on the epidemiology and biological relationships. Obes. Rev. 2020. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Wang, Z.; Wang, S.; Ye, Y.; Luo, D.; Wan, L.; Yu, A.; Sun, L.; Tesfaye, S.; Meng, Q.; et al. The impact of type 2 diabetes and its management on the prognosis of patients with severe COVID-19. J. Diabetes 2020. [Google Scholar] [CrossRef] [PubMed]
- Ko, J.Y.; Danielson, M.L.; Town, M.; Derado, G.; Greenlund, K.J.; Daily Kirley, P.; Alden, N.B.; Yousey-Hindes, K.; Anderson, E.J.; Ryan, P.A.; et al. Risk Factors for COVID-19-associated hospitalization: COVID-19-Associated Hospitalization Surveillance Network and Behavioral Risk Factor Surveillance System. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Wargny, M.; Gourdy, P.; Ludwig, L.; Seret-Bégué, D.; Bourron, O.; Darmon, P.; Amadou, C.; Pichelin, M.; Potier, L.; Thivolet, C.; et al. Type 1 Diabetes in People Hospitalized for COVID-19: New Insights from the CORONADO Study. Diabetes Care 2020. [Google Scholar] [CrossRef]
- Xie, J.; Covassin, N.; Fan, Z.; Singh, P.; Gao, W.; Li, G.; Kara, T.; Somers, V.K. Association between Hypoxemia and Mortality in Patients with COVID-19. Mayo Clin. Proc. 2020, 95, 1138–1147. [Google Scholar] [CrossRef]
- Yan, Y.; Yang, Y.; Wang, F.; Ren, H.; Zhang, S.; Shi, X.; Yu, X.; Dong, K. Clinical characteristics and outcomes of patients with severe covid-19 with diabetes. BMJ Open Diabetes Res. Care 2020, 8. [Google Scholar] [CrossRef]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk stratification of patients admitted to hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Development and validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef]
- SPF Le Poids du Diabète en France en 2016. Synthèse Epidémiologique. Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/diabete/documents/rapport-synthese/le-poids-du-diabete-en-france-en-2016.-synthese-epidemiologique (accessed on 25 August 2020).
- Wynants, L.; Calster, B.V.; Collins, G.S.; Riley, R.D.; Heinze, G.; Schuit, E.; Bonten, M.M.J.; Damen, J.A.A.; Debray, T.P.A.; Vos, M.D.; et al. Prediction models for diagnosis and prognosis of covid-19: Systematic review and critical appraisal. BMJ 2020, 369. [Google Scholar] [CrossRef] [Green Version]
- Perlini, S.; Canevari, F.; Cortesi, S.; Sgromo, V.; Brancaglione, A.; Contri, E.; Pettenazza, P.; Salinaro, F.; Speciale, F.; Sechi, G.; et al. Emergency Department and Out-of-Hospital Emergency System (112-AREU 118) integrated response to Coronavirus Disease 2019 in a Northern Italy centre. Intern. Emerg. Med. 2020, 15, 825–833. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Data Available | All (n = 344) | Outpatients (n = 159) | Inpatients (n = 185) | p |
|---|---|---|---|---|---|
| Sex male/female | 344 | 204/140 (59.3%) | 89/70 (56%) | 115/70 (62.1%) | NS |
| Age (years) | 344 | 62.1 ± 14.0 | 55.2 ± 12.6 | 68 ± 12.6 | <0.0001 |
| <55 years | 100 (29.1%) | 77 (48.4%) | 23 (12.4%) | <0.0001 | |
| 55–64 years | 94 (27.3%) | 46 (28.9%) | 48 (25.9%) | ref | |
| 65–74 years | 82 (23.8%) | 29 (18.2%) | 53 (28.6%) | 0.07 | |
| ≥75 years | 68 (19.8%) | 7 (4.4%) | 61 (33%) | <0.0001 | |
| BMI (kg/m2) | 308 | 29.5 ± 6.6 | 29 ± 5.3 | 29.8 ± 7.5 | NS |
| <25 kg/m2 | 72 (23.4%) | 31 (21.7%) | 41 (24.8%) | NS | |
| 25–29.9 kg/m2 | 114 (37%) | 58 (40.6%) | 56 (33.9%) | NS | |
| 30–39.9 kg/m2 | 101 (32.8%) | 49 (34.3%) | 52 (31.5%) | NS | |
| ≥40 kg/m2 | 21 (6.8%) | 5 (3.5%) | 16 (9.7%) | 0.030 | |
| Autonomy | 344 | <0.0001 | |||
| Autonomous | 307 (89.2%) | 159 (100%) | 148 (80%) | ||
| Non-autonomous | 37 (10.8%) | 0 (0%) | 37 (20%) | ||
| Ethnicity | 292 | 0.010 | |||
| EU | 103 (35.3%) | 43 (28.3%) | 60 (42.9%) | ref | |
| MENA | 123 (42.1%) | 75 (49.3%) | 48 (34.3%) | 0.004 | |
| AC | 64 (21.9%) | 34 (22.4%) | 30 (21.4%) | 0.153 | |
| AS | 2 (0.7%) | 0 (0%) | 2 (0.7%) | NA | |
| Hypertension | 343 | 221 (64.4%) | 70 (44.3%) | 151 (81.6%) | <0.0001 |
| Dyslipidemia | 342 | 139 (40.6%) | 49 (30.8%) | 90 (49.2%) | 0.001 |
| Tobacco use | 320 | <0.0001 | |||
| Never | 236 (73.8%) | 136 (85.5%) | 100 (62.1%) | ||
| Former | 56 (17.5%) | 6 (3.8%) | 50 (31.1%) | ||
| Current | 28 (8.8%) | 17 (10.7%) | 11 (6.8%) | ||
| Type of diabetes | 344 | <0.0001 | |||
| Type 1 | 20 (5.8%) | 18 (11.3%) | 2 (1.1%) | ||
| Type 2 | 324 (94.2%) | 141 (88.7%) | 183 (98.9%) | ||
| Diabetes duration | 267 | 10.8 ± 8.8 | 9.1 ± 8 | 12.4 ± 9.2 | 0.002 |
| HbA1c (%) | 229 | 7.7 ± 1.7 | 7.5 ± 1.6 | 7.8 ± 1.7 | 0.100 |
| Severe hypoglycemia | 285 | 12 (4.2%) | 1 (0.7%) | 12 (4.2%) | 0.006 |
| Microvascular complications | 315 | 109 (34.6%) | 23 (16.7%) | 86 (48.6%) | <0.0001 |
| Severe diabetic retinopathy | 294 | 14 (4.7%) | 6 (4.7%) | 8 (4.8%) | NS |
| Diabetic kidney disease | 344 | 104 (30.2%) | 21 (13.2%) | 83 (44.9%) | <0.0001 |
| History of diabetic foot ulcer | 344 | 6 (1.7%) | 2 (1.3%) | 4 (2.2%) | NS |
| Macrovascular complications | 342 | 71 (20.8%) | 14 (8.9%) | 57 (31%) | <0.0001 |
| Ischemic heart disease | 342 | 58 (17%) | 10 (6.3%) | 48 (26.2%) | <0.0001 |
| Cerebrovascular disease | 338 | 21 (6.1%) | 5 (3.2%) | 16 (8.7%) | 0.040 |
| Peripheral artery disease | 340 | 14 (4.1%) | 2 (1.3%) | 12 (6.5%) | 0.020 |
| Comorbidities | |||||
| CKD * | 331 | 49 (13.8%) | 1 (0.7%) | 48 (26%) | <0.0001 |
| Dialysis | 344 | 8 (2.3%) | 0 (0%) | 8 (4.3%) | 0.010 |
| Heart failure | 340 | 22 (6.5%) | 5 (3.1%) | 17 (9.4%) | 0.030 |
| Sleep apnea | 321 | 37 (11.5%) | 9 (6.2%) | 37 (11.5%) | 0.010 |
| Respiratory failure | 342 | 21 (6.1%) | 3 (1.9%) | 18 (9.8%) | 0.003 |
| COPD | 343 | 16 (4.7%) | 2 (1.3%) | 14 (7.6%) | 0.005 |
| Active cancer | 341 | 12 (3.5%) | 1 (0.6%) | 11 (6%) | 0.007 |
| Transplant | 344 | 4 (1.2%) | 1 (0.6%) | 3 (1.6%) | NS |
| NAFLD or liver cirrhosis | 337 | 24 (7%) | 12 (7.5%) | 12 (6.7%) | NS |
| Bariatric surgery | 344 | 3 (0.9%) | 2 (1.3%) | 1 (0.5%) | NS |
| Treatments | |||||
| Insulin | 337 | 104 (30.9%) | 37 (23.7%) | 67 (37%) | 0.010 |
| Basal bolus regimen | 333 | 66 (19.8%) | 26 (16.9%) | 40 (22.3%) | 0.012 |
| Metformin | 339 | 214 (63.1%) | 104 (67.1%) | 110 (59.8%) | NS |
| DPP4-Inhibitors | 340 | 79 (23.2%) | 37 (23.7%) | 42 (22.8%) | NS |
| GLP1-RA | 340 | 38 (11.2%) | 17 (10.9%) | 21 (11.4%) | NS |
| Glinides | 339 | 35 (10.3%) | 13 (8.4%) | 22 (12%) | NS |
| Sulfonylurea | 339 | 72 (21.2%) | 33 (21.3%) | 39 (21.2%) | NS |
| Anti-platelet agent | 341 | 92 (27%) | 19 (12.1%) | 73 (39.7%) | <0.0001 |
| ACE inhibitors and/or ARBs | 341 | 172 (50.4%) | 53 (33.8%) | 119 (64.7%) | <0.0001 |
| Diuretics | 340 | 76 (22.4%) | 23 (14.7%) | 53 (28.8%) | 0.003 |
| Statins | 341 | 115 (33.7%) | 40 (25.5%) | 75 (40.8%) | 0.004 |
| Anticoagulant | 341 | 28 (8.1%) | 4 (2.6%) | 24 (13%) | 0.001 |
| Variable | Data Available | All (n = 344) | Oupatients (n = 159) | Inpatients (n = 185) | p |
|---|---|---|---|---|---|
| Positive SARS-CoV-2-PCR | 344 | 330 (96%) | 158 (99.4%) | 172 (93%) | 0.002 |
| Typical CT signs | 288 | 246 (85.4%) | 96 (78%) | 150 (88%) | |
| limited | 87 (35.3%) | 59 (61.5%) | 28 (19%) | <0.05 | |
| limited to intermediate | 4 (1.6%) | 0 (0%) | 4 (2.6%) | NS | |
| intermediate | 96 (39%) | 35 (36.5%) | 61 (41%) | NS | |
| intermediate to severe | 8 (3.2%) | 0 (0%) | 8 (5.3%) | NS | |
| severe | 51 (2.2%) | 2 (2%) | 49 (32.1%) | <0.05 | |
| COVID-19 symptoms | 343 | 324 (94.5%) | 144 (90.6%) | 180 (97.8%) | 0.004 |
| Fever | 340 | 165 (48.5%) | 47 (29.6%) | 118 (65.2%) | <0.0001 |
| Cough | 340 | 217 (63.8%) | 92 (57.9%) | 125 (69.1%) | 0.040 |
| Dyspnea | 343 | 133 (38.8%) | 27 (17%) | 106(57.6%) | <0.0001 |
| Cephalalgia | 339 | 77 (22.7%) | 51 (32.1%) | 26 (14.4%) | <0.0001 |
| Anosmia and/or agueusia | 340 | 115 (33.4%) | 85 (53.5%) | 30 (16.6%) | <0.0001 |
| Fatigue | 340 | 205 (60.3%) | 80 (50.3%) | 125 (69.1%) | 0.001 |
| Rhinitis and/or pharyngeal symptoms | 340 | 69 (20.3%) | 55 (34.6%) | 14 (7.7%) | <0.0001 |
| Digestive disorder | 340 | 77 (22.6%) | 31 (19.5%) | 46 (25.4%) | NS |
| Time between symptoms and first day hospital or consultations | 332 | 6 ± 4.6 | 5.8 ± 4.5 | 6.2 ± 4.6 | 0.002 |
| Secondary infection | 336 | 19 (5.7%) | 0 (0%) | 19 (10.7%) | <0.0001 |
| Ketosis | 340 | 7 (2.1%) | 2 (1.3%) | 5 (2.8%) | NS |
| Peripheral oxygen saturation (%) | 313 | 94.3 ± 6.7 | 97.3 ± 1.5 | 91.6 ± 8.3 | <0.0001 |
| Biology at admission | |||||
| Hemoglobin (g/dL) | 330 | 13.4 ± 1.8 | 13.8 ± 1.5 | 13.1 ± 2.0 | <0.0001 |
| White cell count (G/L) | 330 | 6.6 ± 2.7 | 6.0 ± 1.7 | 7.0 ± 3.2 | <0.0001 |
| Lymphocyte count (G/L) | 311 | 1.5 ± 0.9 | 1.8 ± 0.8 | 1.2 ± 0.9 | <0.0001 |
| Neutrophil count (G/L) | 311 | 4.4 ± 2.4 | 3.6 ± 1.5 | 5.1 ± 2.8 | <0.0001 |
| Eosinophil count (G/L) | 311 | 0.02 (0–0.07) | 0.07 ± 0.1 | 0.04 ± 0.144 | NS |
| Platelet count (103/mm3) | 330 | 225 ± 85 | 244 ± 83 | 211 ± 84 | <0.0001 |
| eGFR (/min) | 331 | 77 ± 28.8 | 91.8 ± 21.7 | 66.2 ± 28.7 | <0.0001 |
| Admission plasma glucose (mmol/L) | 324 | 10 ± 5.2 | 9.2 ± 4.2 | 10.7 ± 5.8 | 0.010 |
| ASAT (UI/L) | 292 | 44 ± 30 | 34 ± 18 | 50 ± 35 | <0.0001 |
| ALAT (UI/L) | 292 | 38 ± 28 | 39 ± 26 | 37 ± 30 | NS |
| GGT (UI/L) | 292 | 44 (26–69) | 57 ± 58 | 73 ± 123 | NS |
| CRP (mg/L) | 299 | 32 (5.8–87) | 18.9 ± 33.6 | 88. ± 81.8 | <0.0001 |
| CPK (UI/L) | 280 | 100 (59–191) | 77 (56–134) | 121 (67–257) | 0.001 |
| LDH (UI/L) | 269 | 304 ± 138 | 232.6 ± 56 | 351.2 ± 155 | <0.0001 |
| Albumin (g/L) | 211 | 38 ± 6 | 43 ± 4 | 37 ± 5 | <0.0001 |
| AUC | OR | 95% CI | β Coefficient | p | |
|---|---|---|---|---|---|
| Model 1—Basic medical history | 0.814 | ||||
| Age | 1.07 | (1.04–1.10) | 0.07 | <0.001 | |
| Sex | 0.71 | (0.41–1.23) | −0.34 | 0.22 | |
| Type of diabetes | 2.99 | (0.58–15.44) | 1.10 | 0.19 | |
| Hypertension | 2.94 | (1.65–5.25) | 1.09 | <0.001 | |
| COPD | 5.18 | (0.94–28.43) | 1.64 | 0.06 | |
| BMI (< or ≥ 40) | 3.83 | (1.20–12.22) | 1.34 | 0.02 | |
| Model 2—Medical history and biological data at first examination | 0.860 | ||||
| Age | 1.07 | (1.05–1.10) | 0.07 | <0.001 | |
| Sex | 0.63 | (0.35–1.14) | −0.45 | 0.13 | |
| Type of diabetes (T2D vs T1D) | 3.94 | (0.68–22.9) | 1.37 | 0.13 | |
| Hypertension | 3.91 | (2.08–7.35) | 1.36 | <0.001 | |
| BMI (< or ≥ 40) | 4.39 | (1.28–15.01) | 1.48 | 0.02 | |
| CKD | 28.1 | (3.55–222.33) | 3.34 | 0.002 | |
| Plasma glucose at admission | 1.14 | (1.07–1.22) | 0.13 | <0.001 | |
| Model 3—Medical history and long-term plasma glucose | 0.830 | ||||
| Age | 1.08 | (1.04–1.12) | 0.08 | <0.001 | |
| Sex | 0.62 | (0.30–1.28) | −0.47 | 0.2 | |
| Type of diabetes | 3.83 | (0.77–82.54) | 2.08 | 0.08 | |
| Hypertension | 3.82 | (1.79–8.15) | 1.34 | <0.001 | |
| BMI (< or ≥ 40) | 5.43 | (0.81–36.45) | 1.69 | 0.08 | |
| HbA1c | 1.02 | (0.80–1.29) | 0.02 | 0.88 | |
| Plasma glucose at admission | 1.12 | (1.02–1.24) | 0.18 | 0.02 | |
| Model 4—Medical history and antidiabetic treatment characteristics | 0.825 | ||||
| Age | 1.07 | (1.03–1.09) | 0.06 | <0.001 | |
| Sex | 0.67 | (0.37–1.21) | −0.41 | 0.18 | |
| Type of diabetes | 24.51 | (1.95–307.56) | 3.20 | 0.01 | |
| Hypertension | 2.68 | (1.43–5.05) | 0.99 | 0.002 | |
| BMI | 4.72 | (1.26–17.65) | 1.55 | 0.02 | |
| Severe hypoglycemia | 7.12 | (0.55–91.58) | 1.96 | 0.13 | |
| Insulin treatment | 2.49 | (1.20–5.17) | 0.91 | 0.01 | |
| Model 5—Medical history and diabetes complications | 0.831 | ||||
| Age | 1.05 | (1.03–1.08) | 0.05 | <0.001 | |
| Sex | 0.83 | (0.46–1.49) | −0.19 | 0.53 | |
| Type of diabetes | 4.24 | (0.78–23) | 1.44 | 0.09 | |
| Hypertension | 2.29 | (1.23–4.28) | 0.83 | 0.01 | |
| BMI (< or ≥ 40) | 4.07 | (1.26–13.14) | 1.40 | 0.02 | |
| Microangiopathy | 2.11 | (1.10–4.05) | 0.74 | 0.02 | |
| Macroangiopathy | 3.35 | (1.50–7.52) | 1.21 | 0.003 | |
| Model 6—Medical history and data at first examination | 0.910 | ||||
| Age | 1.03 | (1.00–1.06) | 0.03 | 0.03 | |
| Sex | 0.92 | (0.46–1.84) | −0.08 | 0.82 | |
| Type of diabetes | 45.34 | (2.96–7033.84) | 3.81 | <0.001 | |
| Hypertension | 3.51 | (1.63–7.90) | 1.25 | <0.001 | |
| BMI (< or ≥ 40) | 4.14 | (0.92–21.17) | 1.42 | 0.06 | |
| Peripheral oxygen saturation | 0.58 | (0.47–0.69) | −0.54 | <0.001 | |
| Insulin treatment | 3.98 | (1.82–9.02) | 1.38 | <0.001 | |
| Model 7- Clinical model simplified | 0.910 | ||||
| Age | 1.03 | (1.01–1.06) | 0.03 | 0.01 | |
| Type of diabetes | 52.39 | (3.42–8067.31) | 3.95 | <0.001 | |
| Hypertension | 3.35 | (1.66–7) | 1.21 | <0.001 | |
| Peripheral oxygen saturation | 0.56 | (0.46–0.66) | −0.59 | <0.001 | |
| Insulin treatment | 3.70 | (1.75–8.09) | 1.31 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lasbleiz, A.; Cariou, B.; Darmon, P.; Soghomonian, A.; Ancel, P.; Boullu, S.; Houssays, M.; Romain, F.; Lagier, J.C.; Boucekine, M.; et al. Phenotypic Characteristics and Development of a Hospitalization Prediction Risk Score for Outpatients with Diabetes and COVID-19: The DIABCOVID Study. J. Clin. Med. 2020, 9, 3726. https://doi.org/10.3390/jcm9113726
Lasbleiz A, Cariou B, Darmon P, Soghomonian A, Ancel P, Boullu S, Houssays M, Romain F, Lagier JC, Boucekine M, et al. Phenotypic Characteristics and Development of a Hospitalization Prediction Risk Score for Outpatients with Diabetes and COVID-19: The DIABCOVID Study. Journal of Clinical Medicine. 2020; 9(11):3726. https://doi.org/10.3390/jcm9113726
Chicago/Turabian StyleLasbleiz, Adèle, Bertrand Cariou, Patrice Darmon, Astrid Soghomonian, Patricia Ancel, Sandrine Boullu, Marie Houssays, Fanny Romain, Jean Christophe Lagier, Mohamed Boucekine, and et al. 2020. "Phenotypic Characteristics and Development of a Hospitalization Prediction Risk Score for Outpatients with Diabetes and COVID-19: The DIABCOVID Study" Journal of Clinical Medicine 9, no. 11: 3726. https://doi.org/10.3390/jcm9113726