1. Introduction
Anabolic androgenic steroids (AASs) are widely used illicitly to improve body appearance and increase strength [
1], but they can lead to adverse side effects on immune function [
2]. The link between COVID-19 and AASs has not been extensively documented to date. The only two references to the topic are results published in a cross-sectional study on 39 current AASs users (of 520 total study participants) [
3] and in a case report on a severe COVID-19 male patient using AASs [
4]. These data appear to be supported by the link between androgen signaling and SARS-CoV-2 infectivity, and point to AASs as a risk factor for severe COVID-19.
The aim of the study was to analyze the autopsy results of a young bodybuilder patient, who consumed AASs regularly and was affected by a severe form of COVID-19.
2. Materials and Methods
Histopathology. For the histopathological examination of the organ fragments collected at autopsy, the samples were fixed in formaldehyde 7% for 5 days, after which the samples were oriented and placed in cassettes. Tissue processing was performed using a vacuum infiltration processor, Tissue-Tek VIP 5 Jr (Sakura, Alphen aan den Rijn, The Netherlands). Paraffin embedding and sectioning were performed using the Tissue-Tek TEC 6 system (Sakura, Alphen aan den Rijn, The Netherlands) and Accu-Cut SRM 200 Rotary Microtome (Sakura, Alphen aan den Rijn, The Netherlands). Slide staining was performed using the automated slide stainer Tissue-Tek Prisma Plus (Sakura, Alphen aan den Rijn, The Netherlands) according to the internal staining protocol, using Mayer Modified Hematoxylin (Titolchimica, Rovigo, Italy) and Eosin solution (10 g Eosin B in 1000 mL distilled water).
Immunohistochemistry was performed automatically on 3-μm-thick sections of formalin-fixed and paraffin-embedded tissues with MD Stainer (Vitro Master Diagnostica®, Granada, Spain) using ethylenediaminetetraacetic acid (EDTA), at pH = 9, for antigen retrieval. For the immunohistochemical assessment, we used Anti-SARS Coronavirus NP Mouse anti-Virus antibody (clone B46F, Invitrogen, Waltham, Massachusetts, USA) at a 1:100 dilution, and anti-ACE antibody (clone15348, Abcam, Cambridge, UK) at 1:100 dilution.
Microscopic examination was performed by an experienced pathologist (D.G.) using an Olympus BX46 clinical microscope (Olympus Europe SE & Co, Hamburg, Germany) with dedicated image acquisition camera and software. All sections were examined at 400× magnification.
Molecular biology. During autopsy, 3 lung fragments were collected to perform the SARS-CoV-2 RT-PCR test. Total nucleic acids isolation was performed with MasterPure™ Complete DNA and RNA Purification Kit (EPICENTRE Biotechnologies, Madison, WI, USA), according to the manufacturer’s instructions, using the protocol for total nucleic acids purification from tissue samples. A Pearl Nanophotometer (Implen GmbH, Munich, Germany) was engaged in determining the DNA and RNA concentration and purity. The RNA sample was amplified on a QuantStudio™ 5 RT-PCR System (Thermo Fisher Scientific Inc., Waltham, MA, USA) after reverse transcription, using aSARS-CoV-2 Real-TM kit (Sacace Biotechnologies, Como, Italy). This multiplex RT-PCR assay uses four simultaneous amplification reactions: those of the E gene region common for all SARS-like coronaviruses (FAM channel), the specific SARS-CoV-2 E gene (ROX channel) and the specific SARS-CoV-2 N gene (Cy5 channel), as well as the amplification of the nucleic acid sequence of the Internal Control-RNA (HEX channel). The assay also included a positive control of amplification (cDNA C+). The following program was used: reverse transcription for 20 min at 35 °C, initial denaturation for 5 min at 94 °C, 5 amplification cycles (10 s at 94 °C and 25 s at 64 °C) followed by 45 amplification cycles (10 s at 94 °C and 25 s at 64 °C with fluorescence detection).
Using the initial solution of isolated total nucleic acids, the identification of SARS-CoV-2 variant was performed. RNA preparation and amplification were carried out in accordance with protocols published by the ARTIC network, using the V3 version of the ARTIC primer set from Integrated DNA Technologies (Coralville, IA, USA) to create tiled amplicons across the SARS-CoV-2 genome. Libraries were prepared using the Nextera DNA Flex library preparation kit and MiSeq reagent cartridge V2 (Illumina, San Diego, CA, USA).
Using the same initial solution, the identification of HLA-A, B, C, DRB1 and DQB1 was performed. HLA-FluoGene ABC kit and HLA-FluoGene DRDQ kit (inno-train Diagnostik GmbH, Kronberg, Germany) were used according to the manufacturer’s instructions, based on the Sequence Specific Priming Polymerase Chain Reaction (SSP-PCR). DNA amplification was carried out on a G-Storm thermal cycler (Gene Technologies Ltd., Essex, UK) and the mixture containing the extracted DNA sample was submitted to 40 amplification cycles (15 s at 96 °C and 60 s at 60 °C) after an initial denaturation step for 2 min at 95 °C. Detection of the PCR products was performed by measuring fluorescence signals on a FluoVista Analyzer (inno-train Diagnostik GmbH, Kronberg, Germany), the endpoint fluorescence of the various fluorochromes before and after PCR was automatically calculated using the FluoGene analysis software.
3. Case Presentation
A 34-year-old patient, a fitness and bodybuilding trainer, was found by the ambulance in cardio-respiratory arrest in his home. The patient did not respond to resuscitation maneuvers. A medico-legal autopsy was requested to establish the causes of death.
From the postmortem heteroanamnesis, the following information was recorded:
- -
4 days before death, the patient presented infectious symptomatology with sudden onset (altered general condition, fever 38 °C, curvature, nausea, vomiting, dry cough, dyspnea whose intensity increased progressively); about 15 min before death, the patient presented anxiety, obnubilation, severe dyspnea; death occurred suddenly;
- -
3 days before the onset of the mentioned symptomatology, the patient encountered COVID-19-positive subjects in the gym room;
- -
during the 4 days of illness, the patient self-medicated with paracetamol (3–4 tablets/day), ibuprofen 400 mg (1–2 tablets/day), aspirin in antiplatelet doses (2 tablets/day); the patient refused to be medically evaluated during the illness;
- -
cardiovascular pathology was noted in the patient’s family history—essential arterial hypertension in both parents and polyglobulia (father);
- -
the patient’s personal pathological history was essential hypertension grade II (highest value of Blood Pressure 180/90 mmHg), controlled under monotherapy with bisoprolol 5 mg/day, frequent palpitations with the subjective perception of an irregular heart rhythm, tachycardia, visible apex shock in the left V intercostal space on the medio-clavicular line in orthostatism;
- -
the patient had been constantly practicing strength sports (powerlifting and bodybuilding) for the past 16 years. To improve his performance, the patient had used AASs in a continuous cycle since the age of 18. In the last 6 months before his death, the patient had used Sustanon 250 mg/mL (3 doses/week: Monday, Wednesday, Friday), Nandrolone decanoate 100 mg/mL (administration rate identical to Sustanon), Trenbolone acetate 100 mg/mL alternatively with Methenolon enanthate (2 doses/week). The patient also used, more or less regularly, fast-acting insulin, growth hormones and derivatives (GHRP-6 peptides, ipamorelin, vermotropin), multivitamins, omega 3-6-9 fatty acids (3–4 capsules daily), linseed oil, high molecular weight carbohydrate powder, isolated protein powder 2 g/body kg/day, creatine, caffeine-based energy drinks. In the last 2–3 years, the patient was doing 5 bodybuilding workouts/week, without cardio type workouts, and his diet consisted of 3 main meals with a total nutritional value of less than 3000 kcal.
Macroscopic autopsy findings. Necropsy was performed 24 h postmortem. On external examination—male corpse, 165 cm tall, 85 kg, BMI 31.22, marked muscle hypertrophy (
Figure 1A,B), no signs of putrefaction, with “cape” cyanosis (
Figure 1A).
The lungs had increased weight (right lung 965 g, left lung 790 g), violet color; on the pleuro-pulmonary surface, bilaterally, multiple reddish hematic suffusions, with a diameter of 0.1–0.2 cm, could be detected (
Figure 1C). When palpating the lungs, increased consistency was perceived, without crepitations. In the section, a compact, glossy appearance was observed; a significant amount of dark red blood and foamy, pinkish fluid oozes (
Figure 1D).
The aorta showed numerous yellowish atherosclerotic plaques, raised on the surface of the intima (
Figure 1E). The heart (460 g) showed myocardial hypertrophy (
Figure 1F,G), the wall of the left ventricle had a maximum thickness of 3 cm, and the interventricular septum—2.5 cm. On the cross-section, a gray-whitish area of sclerosis (old myocardial infarction,
Figure 1G) could be identified on the left ventricular wall. The liver had a significantly increased weight (2735 g) and was yellowish-brown in color (
Figure 1H,I). The pancreas also showed significantly increased dimensions (weight 145 g) (
Figure 1J).
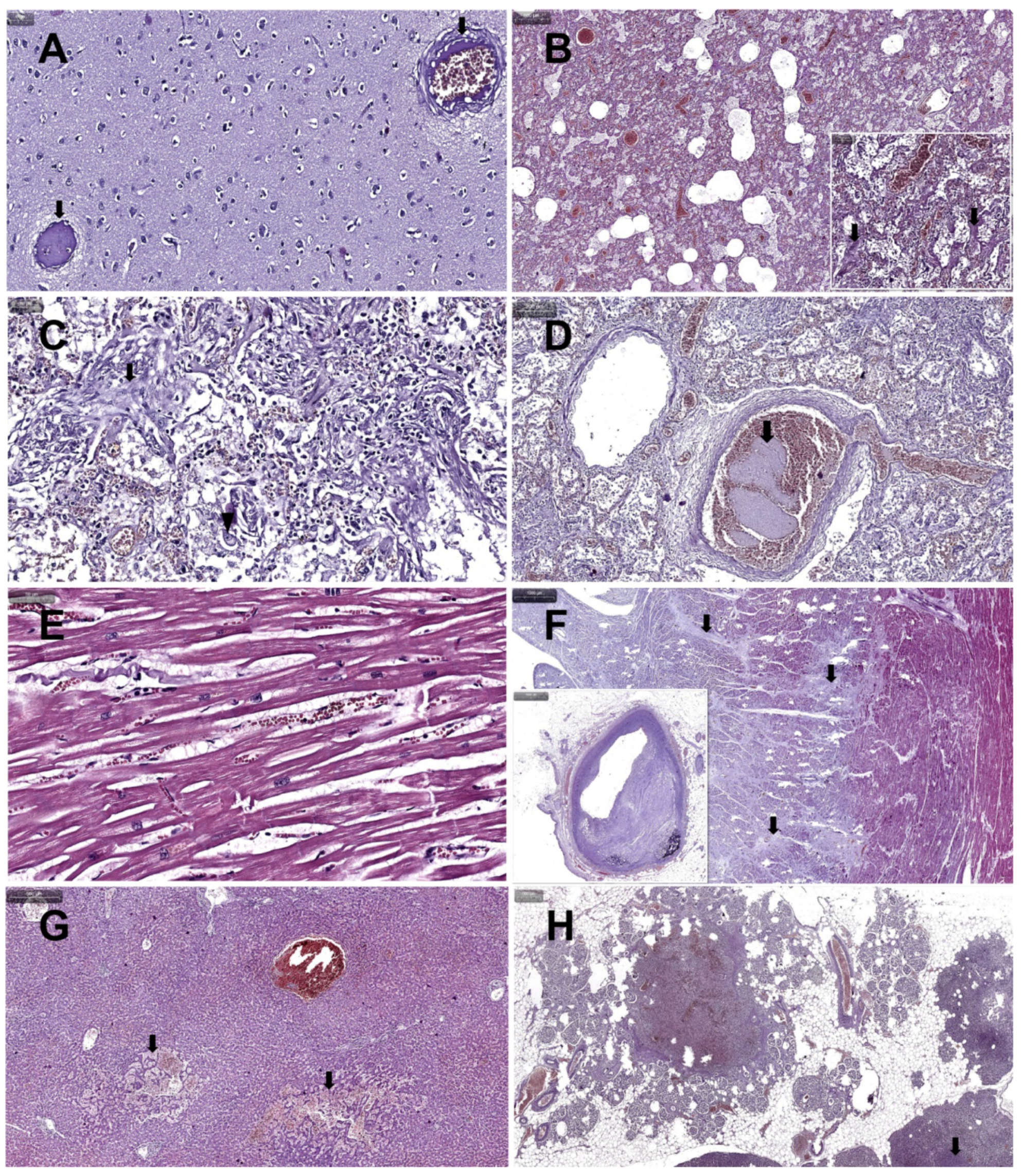
The results of the histopathological examination showed microthrombi with endothelitis (arrows) in cerebral tissue, on a cerebral edema background (
Figure 2A), in pulmonary tissue—stasis, emphysema and massive pulmonary edema (
Figure 2B) with diffuse alveolar damage (DAD) grade 1 (
Figure 2B detail arrows), focal organizing pneumonia (
Figure 2C arrow) and alveolar giant macrophages with nuclear viral inclusion (
Figure 2C arrow head), pulmonary thromboembolism (
Figure 2D arrow). The heart showed hypertrophic myocadiac muscular fibers (
Figure 2E), old subendocardial myocardial infarction (
Figure 2F arrows), associated with significant coronary artery occlusion by advanced atheromatous plaque (
Figure 2F insert). The liver presented hepatic peliosis (
Figure 2G arrows), and the pancreas—severe nesidioblastosis and multifocal necrosis (
Figure 2H).
Results of the immunohistochemical examinations are presented in the
Table 1.
Molecular biology. The RNA test was positive for SARS-CoV-2, and the amplification of all three targets were observed: SARS-like coronaviruses gene (Ct = 25,274), E gene (Ct = 21,848) and N gene (Ct = 25,915). The test for identification of SARS-CoV-2 variant indicated the genetic line B.1.258.
The following HLA allele were identified: A*03, A*25, B*18, B*35, C*04, C*12, DRB1*04, DRB1*15, DQB1*03, DQB1*06.
4. Discussion
Genetic data. Data literature show that the HLA allele pairs identified by us in the studied patient correlate with severe forms of the disease (HLA-DRB1*04) [
5], and prolonged duration of the disease (DQB1*03:02) [
6]. In a group of 99 Italian patients affected by a severe or extremely severe form of COVID-19, HLA allele frequency distribution demonstrated a significant association for HLA-DRB1*15:01 and HLA-DQB1*06:02 compared to a reference group of 1017 Italian individuals [
7]. One study gives a higher rate of the HLA-A*03 allele in COVID-19 patients than in healthy controls [
8] and another study showed a positive log-linear correlation of A*25 allele with COVID-19 incidence rate [
9]. Inspection of COVID-19 disease severity outcomes reveal significant risk associations with C*04:01 [
10,
11].
The genetic line identified in our case, B.1.258, had been circulated in Central Europe since August 2020, long before the import of B.1.1.7 [
12].
Testosterone and COVID-19. Synthetic analogues of testosterone are the most widely used AASs [
13].
Regarding the correlation between testosterone levels and severe forms of COVID-19, a prospective study of 358 COVID-19 patients described a correlation between low serum testosterone and a poor prognosis, finding that low testosterone was linked to more severe forms of COVID -19, a need for intensive care and death [
14]. However, that study did not establish whether initially low testosterone predisposed patients to worse COVID -19-related outcomes, or whether the infection with SARS-CoV-2 caused lower testosterone levels, with more severe infections potentially leading to larger decreases in testosterone. Another study, on a smaller sample of 81 COVID-19 patients, identified the same connection between low testosterone levels and poorer COVID-19 outcomes, albeit without reaching statistical significance [
15].
However, the link between androgen signaling and SARS-CoV-2 infectivity has been established and is believed to explain, at least in part, why men tend to have more severe forms of COVID-19 compared to women [
16]. Although the determination of serum testosterone concentration was not performed in the case of our patient, its values were certainly above the physiological limit at the time of SARS-CoV-2 infection, negatively influencing the patient’s immune system [
17,
18,
19].
Authors believe that the thromboembolic phenomena of this case (
Figure 2A,D) are due to both AASs and a background of a genetic predisposition (father with polyglobulia) and to the COVID-19 infection. Testosterone causes erythrocytosis, a well-established side effect [
20]. Although the mechanism linking thromboembolism to AASs abuse has not been elucidated, reviews on this topic present a broad consensus linking AASs abuse to an increased risk of developing thromboembolism, among other cardiovascular disorders [
21,
22]. Another review explains that, although AASs can also lead to enhanced fibrinolysis, their net overall effect remains procoagulant, maintaining consensus with the previously mentioned studies [
23]. On the other hand, the risk of thromboembolism in COVID-19 is already well known [
24,
25].
Testosterone and immunity. Sexual dimorphism in immunity has been widely studied, and the consensus is that females have more active immune systems compared to males, meaning that they are better equipped to combat various infections, while at the same time being more susceptible to autoimmune diseases. This is a result of both hormonal and genetic factors, and their individual contributions could not be fully separated [
26,
27]. A review on the role of testosterone concluded that it has an overall immunosuppressive effect mediated by its action on a host of innate and adaptive immune cells [
28].
The effect of AASs use on immunity has not been widely studied. A small study on 13 healthy bodybuilders using AASs showed marginal reductions in serum IgG, IgA and IgM levels compared to non-AASs users [
29]. Some case studies appear to link AAS-related immunosuppression to increased disease severity in conditions such as severe rhinovirus pneumonia [
30], septic shock with acute respiratory distress syndrome [
31], necrotizing myofasciitis [
32] and recurring herpes zoster ophthalmicus infection [
33].
While the influence of testosterone or AASs on the immune response requires further study, they both have immunosuppressive effects that may reasonably lead to poorer outcomes when fighting infection. Thus, the case studied had a low immune status at the time of infection.
Histopathological changes. Among the cardiovascular disorders caused by AASs abuse, myocardial infarction is widely reported, and is most often triggered by atherosclerosis (
Figure 1E and
Figure 2F), increased thrombogenesis or vasospasms [
34]. In most cases, peliosis hepatis (
Figure 2G) has been associated with long-term AASs use; in the event of intraperitoneal hemorrhages, it can endanger the patient’s life [
35].
Reports of nesidioblastosis (
Figure 2H) in adults are extremely rare. The cause of nesidioblastosis in adults is unknown, but it could either be a genetic defect similar to those causing congenital hyperinsulinism [
36]. In all reports, nesidioblastosis is linked to hyperinsulinism. No reports were found connecting nesidioblastosis to the use of exogenous insulin, AASs or growth hormone. Growth hormones encourage the growth of tissue (
Figure 1H,J) and create a hyperglycemic environment in the body [
37].
The pulmonary histopathological changes observed (
Figure 2B–D) are already known and described in the COVID-19 literature [
38,
39,
40]. The human pancreas can be a target of SARS-CoV-2 infection, and β-cell infection (
Figure 3F) could contribute to the metabolic dysregulation/diabetes observed in patients with COVID-19 [
41]. Studies on necropsic kidney fragments (immunostaining and in situ hybridization) suggest that SARS-CoV-2 is present in various segments of the nephron [
42].
The lack of laboratory examinations and antemortem radio-imaging investigations, as well as the lack of serum determination of the postmortem AASs concentration, represent limitations to our study.
5. Conclusions
In the case analyzed, the severe form of COVID-19 was due to several factors: genetic predisposition, long-term abuse of AASs, which favored the development of a pluriorganic pathological tissue terrain, and recent consumption of AASs, which influenced the immune system at the time of infection. The main reason of death was COVID-19. Severe lung damage was followed by multiple organ failure and death.
Author Contributions
Conceptualization, C.V.S. and I.I.J.; methodology, D.G., D.M., S.Ș., M.L.V., M.L. and M.A.; software, D.G., I.I.J. and V.A.; validation, C.V.S., D.G., M.L.V. and M.L.; formal analysis, I.I.J. and D.M.; investigation, I.I.J., D.G., D.M., M.L.V. and M.L.; resources, V.A. and C.T.; data curation, I.I.J., M.L.V. and M.L.; writing—original draft preparation, I.I.J., V.A., D.G. and M.L.V.; writing—review and editing, S.A. and M.A.; visualization, M.A., S.Ș. and C.T.; supervision, C.V.S. and S.A.; project administration, I.I.J.; funding acquisition, C.V.S. and I.I.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the Guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Iuliu Hatieganu University of Medicine and Pharmacy, Cluj-Napoca, Romania, No. 63/1.03.2022 and with Agreement of the Institute of Legal Medicine, No. 4353/XII/614/25.03.2021.
Informed Consent Statement
Informed consent was obtained from the patient’s next-of-kin after providing information and explaining the purpose and the meaning of the research. Written informed consent was obtained from the patient’s next-of-kin to publish this paper.
Data Availability Statement
The autopsy results are available at the Institute of Legal Medicine in Cluj-Napoca Romania; Contact:
[email protected]. The immunohistochemistry results are available at the Department of Anatomy and Embryology, Iuliu Hatieganu University of Medicine and Pharmacy, Cluj-Napoca, Romania; Contact:
[email protected]. The genetic data and molecular biology results are available at the Department of Cell and Molecular Biology, Iuliu Hatieganu University of Medicine and Pharmacy, Cluj-Napoca, Romania;
[email protected]; The virology analysis results are available at the Viral Respiratory Infections Laboratory, Cantacuzino National Military-Medical Institute for Research and Development, Bucharest, Romania; Contact:
[email protected].
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bonnecaze, A.K.; O’Connor, T.; Aloi, J.A. Characteristics and Attitudes of Men Using Anabolic Androgenic Steroids (AAS): A Survey of 2385 Men. Am. J. Men’s Health 2020, 14, 1557988320966536. [Google Scholar] [CrossRef] [PubMed]
- Marshall-Gradisnik, S.; Green, R.; Brenu, E.; Weatherby, R. Anabolic androgenic steroids effects on the immune system: A review. J. Open Life Sci. 2009, 4, 19–33. [Google Scholar] [CrossRef]
- Althobaiti, Y.S.; Alzahrani, M.S.; Alhumayani, S.M.; Assiry, S.A.; Aljuaid, H.F.; Algarni, M.A. Potential Association between the Use of Anabolic Steroids and COVID-19 Infection. Healthcare 2022, 10, 196. [Google Scholar] [CrossRef] [PubMed]
- Cadegiani, F.; Lin, E.M.; Goren, A.; Wambier, C.G. Potential risk for developing severe COVID-19 disease among anabolic steroid users. BMJ Case Rep. 2021, 14, e241572. [Google Scholar] [CrossRef] [PubMed]
- Langton, D.J.; Bourke, S.C.; Lie, B.A.; Reiff, G.; Natu, S.; Darlay, R.; Burn, J.; Echevarria, C. The influence of HLA genotype on the severity of COVID-19 infection. HLA 2021, 98, 14–22. [Google Scholar] [CrossRef]
- Fischer, J.C.; Schmidt, A.G.; Bölke, E.; Uhrberg, M.; Keitel, V.; Feldt, T.; Jensen, B.; Häussinger, D.; Adams, O.; Schneider, E.M.; et al. Association of HLA genotypes, AB0 blood type and chemokine receptor 5 mutant CD195 with the clinical course of COVID-19. Eur. J. Med. Res. 2021, 26, 107. [Google Scholar] [CrossRef]
- Novelli, A.; Andreani, M.; Biancolella, M.; Liberatoscioli, L.; Passarelli, C.; Colona, V.L.; Rogliani, P.; Leonardis, F.; Campana, A.; Carsetti, R.; et al. HLA allele frequencies and susceptibility to COVID-19 in a group of 99 Italian patients. HLA 2020, 96, 610–614. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; Franco, A.; Barrios, Y.; Cáceres, J.J.; Solé-Violán, J.; Perez, A.; Marcos Y Ramos, J.A.; Ramos-Gómez, L.; Ojeda, N.; et al. HLA genetic polymorphisms and prognosis of patients with COVID-19. Med. Intensiv. 2021, 45, 96–103. [Google Scholar] [CrossRef]
- Correale, P.; Mutti, L.; Pentimalli, F.; Baglio, G.; Saladino, R.E.; Sileri, P.; Giordano, A. HLA-B*44 and C*01 Prevalence Correlates with Covid19 Spreading across Italy. Int. J. Mol. Sci. 2020, 21, 5205. [Google Scholar] [CrossRef]
- Warren, R.L.; Birol, I. Retrospective in silico HLA predictions from COVID-19 patients reveal alleles associated with disease prognosis. MedRxiv 2020. [Google Scholar] [CrossRef]
- Weiner, J.; Suwalski, P.; Holtgrewe, M.; Rakitko, A.; Thibeault, C.; Müller, M.; Patriki, D.; Quedenau, C.; Krüger, U.; Ilinsky, V.; et al. Increased risk of severe clinical course of COVID-19 in carriers of HLA-C*04:01. EClinicalMedicine 2021, 40, 101099. [Google Scholar] [CrossRef]
- Brejová, B.; Boršová, K.; Hodorová, V.; Čabanová, V.; Reizigová, L.; Paul, E.D.; Čekan, P.; Klempa, B.; Nosek, J.; Vinař, T. A SARS-CoV-2 mutant from B.1.258 lineage with ∆H69/∆V70 deletion in the Spike protein circulating in Central Europe in the fall 2020. Virus Genes 2021, 57, 556–560. [Google Scholar] [CrossRef]
- Dotson, J.L.; Brown, R.T. The history of the development of anabolic-androgenic steroids. Pediatr. Clin. N. Am. 2007, 54, 761–769. [Google Scholar] [CrossRef]
- Cinislioglu, A.E.; Cinislioglu, N.; Demirdogen, S.O.; Sam, E.; Akkas, F.; Altay, M.S.; Utlu, M.; Sen, I.A.; Yildirim, F.; Kartal, S.; et al. The relationship of serum testosterone levels with the clinical course and prognosis of COVID-19 disease in male patients: A prospective study. Andrology 2022, 10, 24–33. [Google Scholar] [CrossRef]
- Apaydin, T.; Sahin, B.; Dashdamirova, S.; Dincer Yazan, C.; Elbasan, O.; Ilgin, C.; Bilgin, H.; Cam, H.K.; Bahramzada, G.; Kucuk, A.; et al. The association of free testosterone levels with coronavirus disease 2019. Andrology 2022, 10, 1038–1046. [Google Scholar] [CrossRef]
- Samuel, R.M.; Majd, H.; Richter, M.N.; Ghazizadeh, Z.; Zekavat, S.M.; Navickas, A.; Ramirez, J.T.; Asgharian, H.; Simoneau, C.R.; Bonser, L.R.; et al. Androgen Signaling Regulates SARS-CoV-2 Receptor Levels and Is Associated with Severe COVID-19 Symptoms in Men. Cell Stem Cell 2020, 27, 876–889. [Google Scholar] [CrossRef]
- Mendenhall, C.L.; Grossman, C.J.; Roselle, G.A.; Hertelendy, Z.; Ghosn, S.J.; Lamping, K.; Martin, K. Anabolic steroid effects on immune function: Differences between analogues. J. Steroid Biochem. Mol. Biol. 1990, 37, 71–76. [Google Scholar] [CrossRef]
- Brenu, E.W.; McNaughton, L.; Marshall-Gradisnik, S.M. Is there a potential immune dysfunction with anabolic androgenic steroid use?: A review. Mini Rev. Med. Chem. 2011, 11, 438–445. [Google Scholar] [CrossRef]
- Massart, S.; Redivo, B.; Flamion, E.; Mandiki, S.N.; Falisse, E.; Milla, S.; Kestemont, P. The trenbolone acetate affects the immune system in rainbow trout, Oncorhynchus mykiss. Aquat. Toxicol. 2015, 163, 109–120. [Google Scholar] [CrossRef]
- Ohlander, S.J.; Varghese, B.; Pastuszak, A.W. Erythrocytosis Following Testosterone Therapy. Sex Med. Rev. 2018, 6, 77–85. [Google Scholar] [CrossRef]
- Albano, G.D.; Amico, F.; Cocimano, G.; Liberto, A.; Maglietta, F.; Esposito, M.; Rosi, G.L.; Di Nunno, N.; Salerno, M.; Montana, A. Adverse Effects of Anabolic-Androgenic Steroids: A Literature Review. Healthcare 2021, 9, 97. [Google Scholar] [CrossRef]
- Perry, J.C.; Schuetz, T.M.; Memon, M.D.; Faiz, S.; Cancarevic, I. Anabolic Steroids and Cardiovascular Outcomes: The Controversy. Cureus 2020, 12, e9333. [Google Scholar] [CrossRef]
- Chang, S.; Münster, A.B.; Gram, J.; Sidelmann, J.J. Anabolic Androgenic Steroid Abuse: The Effects on Thrombosis Risk, Coagulation, and Fibrinolysis. Semin. Thromb. Hemost. 2018, 44, 734–746. [Google Scholar] [CrossRef]
- Poor, H.D. Pulmonary Thrombosis and Thromboembolism in COVID-19. Chest 2021, 160, 1471–1480. [Google Scholar] [CrossRef] [PubMed]
- Keane, G.; Dorman, T. Fatal pulmonary thromboembolism in asymptomatic COVID-19. Ir. J. Med. Sci. 2022, 191, 1777–1783. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, R.; Cheung, A.S.; Pang, K.; Saffery, R.; Novakovic, B. Sexual Dimorphism in Innate Immunity: The Role of Sex Hormones and Epigenetics. Front. Immunol. 2021, 11, 604000. [Google Scholar] [CrossRef] [PubMed]
- Jaillon, S.; Berthenet, K.; Garlanda, C. Sexual Dimorphism in Innate Immunity. Clin. Rev. Allergy Immunol. 2019, 56, 308–321. [Google Scholar] [CrossRef] [PubMed]
- Trigunaite, A.; Dimo, J.; Jørgensen, T.N. Suppressive effects of androgens on the immune system. Cell Immunol. 2015, 294, 87–94. [Google Scholar] [CrossRef]
- Calabrese, L.H.; Kleiner, S.M.; Barna, B.P.; Skibinski, C.I.; Kirkendall, D.T.; Lahita, R.G.; Lombardo, J.A. The effects of anabolic steroids and strength training on the human immune response. Med. Sci. Sports Exerc. 1989, 21, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Mayer, K.N.; Wyder, D.; Spasic, D.; Herren, T. Severe rhinovirus pneumonia in a young woman taking performance-enhancing drugs. BMJ Case Rep. 2016, 2016, bcr2015213836. [Google Scholar] [CrossRef] [Green Version]
- Herr, A.; Rehmert, G.; Kunde, K.; Gust, R.; Gries, A. 30-jähriger Bodybuilder mit septischem Schock und ARDS bei Abusus anabolandrogener Steroide [A thirty-year old bodybuilder with septic shock and ARDS from abuse of anabolic steroids]. Anaesthesist 2002, 51, 557–563. [Google Scholar] [CrossRef]
- Bertozzi, G.; Sessa, F.; Maglietta, F.; Cipolloni, L.; Salerno, M.; Fiore, C.; Fortarezza, P.; Ricci, P.; Turillazzi, E.; Pomara, C. Immunodeficiency as a side effect of anabolic androgenic steroid abuse: A case of necrotizing myofasciitis. Forensic. Sci. Med. Pathol. 2019, 15, 616–621. [Google Scholar] [CrossRef]
- LoBue, S.A.; Goldman, A.; Giovane, R.A.; Carlson, S.M.; Bivona, M.; Albear, S.; LoBue, T.D. Recurrent Herpes Zoster Ophthalmicus Preceded by Anabolic Steroids and High-Dose L-Arginine. Case Rep. Ophthalmol. Med. 2020, 2020, 8861892. [Google Scholar] [CrossRef]
- Seara, F.A.C.; Olivares, E.L.; Nascimento, J.H.M. Anabolic steroid excess and myocardial infarction: From ischemia to reperfusion injury. Steroids 2020, 161, 108660. [Google Scholar] [CrossRef]
- Bagheri, S.A.; Boyer, J.L. Peliosis hepatis associated with androgenic-anabolic steroid therapy. A severe form of hepatic injury. Ann. Intern. Med. 1974, 81, 610–618. [Google Scholar] [CrossRef]
- Suchi, M.; MacMullen, C.; Thornton, P.S.; Ganguly, A.; Stanley, C.A.; Ruchelli, E.D. Histopathology of congenital hyperinsulinism: Retrospective study with genotype correlations. Pediatr. Dev. Pathol. 2003, 6, 322–333. [Google Scholar] [CrossRef]
- Brinkman, J.E.; Tariq, M.A.; Leavitt, L.; Sharma, S. Physiology, Growth Hormone. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK482141/ (accessed on 24 June 2022).
- Konopka, K.E.; Nguyen, T.; Jentzen, J.M.; Rayes, O.; Schmidt, C.J.; Wilson, A.M.; Farver, C.F.; Myers, J.L. Diffuse alveolar damage (DAD) resulting from coronavirus disease 2019 Infection is Morphologically Indistinguishable from Other Causes of DAD. Histopathology 2020, 77, 570–578. [Google Scholar] [CrossRef]
- Valdebenito, S.; Bessis, S.; Annane, D.; Lorin de la Grandmaison, G.; Cramer-Bordé, E.; Prideaux, B.; Eugenin, E.A.; Bomsel, M. COVID-19 Lung Pathogenesis in SARS-CoV-2 Autopsy Cases. Front. Immunol. 2021, 12, 735922. [Google Scholar] [CrossRef]
- Jeican, I.I.; Gheban, D.; Barbu-Tudoran, L.; Inișca, P.; Albu, C.; Ilieș, M.; Albu, S.; Vică, M.L.; Matei, H.V.; Tripon, S.; et al. Respiratory Nasal Mucosa in Chronic Rhinosinusitis with Nasal Polyps versus COVID-19: Histopathology, Electron Microscopy Analysis and Assessing of Tissue Interleukin-33. J. Clin. Med. 2021, 10, 4110. [Google Scholar] [CrossRef]
- Müller, J.A.; Groß, R.; Conzelmann, C.; Krüger, J.; Merle, U.; Steinhart, J.; Weil, T.; Koepke, L.; Bozzo, C.P.; Read, C.; et al. SARS-CoV-2 infects and replicates in cells of the human endocrine and exocrine pancreas. Nat. Metab. 2021, 3, 149–165. [Google Scholar] [CrossRef]
- Bouquegneau, A.; Erpicum, P.; Grosch, S.; Habran, L.; Hougrand, O.; Huart, J.; Krzesinski, J.-M.; Misset, B.; Hayette, M.-P.; Delvenne, P.; et al. COVID-19-associated Nephropathy Includes Tubular Necrosis and Capillary Congestion, with Evidence of SARS-CoV-2 in the Nephron. Kidney360 2021, 2, 639–652. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}