Download as pdf or txt
You might also like
- Derain Carla Elize-Group9 DXRDocument6 pagesDerain Carla Elize-Group9 DXRCarla Elize Derain100% (1)
- Form 1Document108 pagesForm 1Asim MohamedNoch keine Bewertungen
- AMBOSS ScholarshipDocument3 pagesAMBOSS ScholarshipEmanuella Gómez Martínez100% (1)
- Pre-Op Case Protocol #4Document2 pagesPre-Op Case Protocol #4IC BNoch keine Bewertungen
- Master of Internal Medicine Logbook1Document112 pagesMaster of Internal Medicine Logbook1alhusseinaliNoch keine Bewertungen
- Notes On History Taking in The Cardiovascular SystemDocument10 pagesNotes On History Taking in The Cardiovascular Systemmdjohar72Noch keine Bewertungen
- Surgery H&P TemplateDocument2 pagesSurgery H&P Templatesjjudge2011100% (1)
- Biochem Finals Module 1 FinalsDocument10 pagesBiochem Finals Module 1 FinalsJeffrey RamosNoch keine Bewertungen
- Pat 2 Medsurg1Document20 pagesPat 2 Medsurg1api-300849832Noch keine Bewertungen
- Cardiology Case 1Document2 pagesCardiology Case 1vil62650% (2)
- Acute Myocardial InfarctionDocument20 pagesAcute Myocardial InfarctionDavid Christian CalmaNoch keine Bewertungen
- Classification of DrugsDocument17 pagesClassification of DrugsBijay Kumar MahatoNoch keine Bewertungen
- Trusted Medical Answers-In Seconds.: General MycologyDocument19 pagesTrusted Medical Answers-In Seconds.: General MycologyntnquynhproNoch keine Bewertungen
- Oral Revalida Im Cases Dec. 12 and 13 2020Document16 pagesOral Revalida Im Cases Dec. 12 and 13 2020Bea Y. Bas-ongNoch keine Bewertungen
- Quizlet PDFDocument191 pagesQuizlet PDFsr100% (1)
- Medical Case 1: Language Centre of Malahayati University at 2010Document16 pagesMedical Case 1: Language Centre of Malahayati University at 2010putri1114Noch keine Bewertungen
- Patient Education ToolkitDocument15 pagesPatient Education ToolkitI Nyoman Gede SemarajanaNoch keine Bewertungen
- Questions and Answers1236Document6 pagesQuestions and Answers1236Potchie PFIZERNoch keine Bewertungen
- Acute Rheumatic Fever PathophysiologyDocument1 pageAcute Rheumatic Fever PathophysiologyMoonyeen Jann Casera BalicNoch keine Bewertungen
- Test Taking NLEDocument4 pagesTest Taking NLEJayvee AmpoNoch keine Bewertungen
- Assessment of The Chest and Lungs: Pat Jackson AllenDocument50 pagesAssessment of The Chest and Lungs: Pat Jackson Allenbuzz Q100% (3)
- Hanson Infectious Diseases - Anamneza I StatusDocument33 pagesHanson Infectious Diseases - Anamneza I StatusSilvia KesegNoch keine Bewertungen
- Portal Hypertension - A Case ReportDocument65 pagesPortal Hypertension - A Case ReportTEAM K 1920Noch keine Bewertungen
- Ent OpdDocument5 pagesEnt OpdRenz Marion Alemania100% (1)
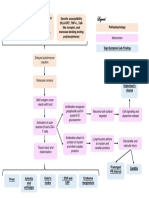
- Pathophysiology of Heart FailureDocument2 pagesPathophysiology of Heart FailureJaysellePuguonTabijeNoch keine Bewertungen
- GI PathoDocument20 pagesGI Pathojutah2013Noch keine Bewertungen
- Ethics Public Health PDFDocument64 pagesEthics Public Health PDFهنادي رازمNoch keine Bewertungen
- Medicine Case Presentation Pneumonia-CVADocument13 pagesMedicine Case Presentation Pneumonia-CVAJonas Dela CruzNoch keine Bewertungen
- Family MedicineDocument5 pagesFamily MedicineDianne SalalilaNoch keine Bewertungen
- Pharmacology Table - GonzalesDocument14 pagesPharmacology Table - GonzalesMark Angelo PonferradoNoch keine Bewertungen
- HyphemaDocument19 pagesHyphemaLiyanti RinceNoch keine Bewertungen
- AnemiaDocument10 pagesAnemiaBia Payawal100% (2)
- Cardiovascular Diseases ListDocument7 pagesCardiovascular Diseases ListAnant SinghNoch keine Bewertungen
- Diarrhea Concept MapDocument1 pageDiarrhea Concept MapIris MambuayNoch keine Bewertungen
- Grand Rounds - Pulmonary EmbolismDocument25 pagesGrand Rounds - Pulmonary EmbolismAdrian CastroNoch keine Bewertungen
- Evaluation of Chest Pain: William Norcross, M.DDocument16 pagesEvaluation of Chest Pain: William Norcross, M.DAbhinit Riddhi100% (1)
- Physical Inactivity: Aging Men Hypertension Smoker ObesityDocument1 pagePhysical Inactivity: Aging Men Hypertension Smoker ObesityKEn PilapilNoch keine Bewertungen
- Case Study PPT Patho NLNGDocument36 pagesCase Study PPT Patho NLNGKate ChavezNoch keine Bewertungen
- Clinical Practice Guidelines: Chronic Suppurative Otitis Media in AdultsDocument28 pagesClinical Practice Guidelines: Chronic Suppurative Otitis Media in Adultsnanu-jenuNoch keine Bewertungen
- Case Study 2Document2 pagesCase Study 2CJ BagasNoch keine Bewertungen
- Drug Overdose and ManagementDocument9 pagesDrug Overdose and ManagementKoRnflakes100% (1)
- Assesment Chest PainDocument9 pagesAssesment Chest PainIpar Day100% (2)
- InfectionDocument42 pagesInfectionAhmad SobihNoch keine Bewertungen
- PericarditisDocument14 pagesPericarditisinterna MANADONoch keine Bewertungen
- Carbuncle, Incision, Drainage, DebridementDocument11 pagesCarbuncle, Incision, Drainage, DebridementAlvin Germo PasuquinNoch keine Bewertungen
- 6 - Ethics + Public Health - 2021 EditionDocument64 pages6 - Ethics + Public Health - 2021 Editiondivyansh77884Noch keine Bewertungen
- MED1 Samplex Rationale 6 - Endocrine DisordersDocument6 pagesMED1 Samplex Rationale 6 - Endocrine DisordersMartina GarciaNoch keine Bewertungen
- Ethic ScenariosDocument28 pagesEthic ScenariosQusaiBadrNoch keine Bewertungen
- Cardiovascular Examination TechniquesDocument36 pagesCardiovascular Examination TechniquesRUTUJA HARISH KSHIRSAGAR100% (1)
- Heart MurmursDocument48 pagesHeart MurmursAhmed T Al-MomtinNoch keine Bewertungen
- Rheumatic Heart Disease AustrliaDocument63 pagesRheumatic Heart Disease AustrliaMuhammad Reza100% (2)
- Shock PresentationDocument20 pagesShock Presentationrosalyn sugayNoch keine Bewertungen
- Blood and Drugs Medicine NotesDocument39 pagesBlood and Drugs Medicine Notesrahuul prasadNoch keine Bewertungen
- Acute Medicine: Shock: Inadequate Tissue and Organ PerfusionDocument3 pagesAcute Medicine: Shock: Inadequate Tissue and Organ Perfusionmyat252Noch keine Bewertungen
- Sample Questions - True Learn Family MedicineDocument11 pagesSample Questions - True Learn Family MedicinelarazahabiNoch keine Bewertungen
- Cerebrovascular Accident (Stroke)Document15 pagesCerebrovascular Accident (Stroke)mesdejen100% (1)
- Answer All The Following Short Essay Questions: (5 Questions)Document5 pagesAnswer All The Following Short Essay Questions: (5 Questions)Soad ShedeedNoch keine Bewertungen
- Triads in MedicineDocument6 pagesTriads in MedicinedeaceNoch keine Bewertungen
- Cardiovascular Physical ExaminationDocument29 pagesCardiovascular Physical ExaminationannisNoch keine Bewertungen
- Coronary ArteriesDocument6 pagesCoronary Arteriesstudy mailNoch keine Bewertungen
- Myocardia IschemiaDocument114 pagesMyocardia Ischemiasara rababahNoch keine Bewertungen
- General Anesthesia: How To Provide General Anesthesia With Brian Warriner, MDDocument34 pagesGeneral Anesthesia: How To Provide General Anesthesia With Brian Warriner, MDSarah RonquilloNoch keine Bewertungen
- Benign Prostatic Hyperplasia Concept MapDocument1 pageBenign Prostatic Hyperplasia Concept MapSarah RonquilloNoch keine Bewertungen
- Drug Index Updated2 2Document104 pagesDrug Index Updated2 2Sarah RonquilloNoch keine Bewertungen
- How To Read An ECGDocument15 pagesHow To Read An ECGSarah Ronquillo100% (1)
- Rigid ProctosigmoidosDocument7 pagesRigid ProctosigmoidosSarah RonquilloNoch keine Bewertungen
- Wpro Iris WhoDocument134 pagesWpro Iris WhoSarah RonquilloNoch keine Bewertungen
- Anesthetic Management in Emergency Exploratory Laparotomy of Perforation Peritonitis in 92 Years Old PatientDocument3 pagesAnesthetic Management in Emergency Exploratory Laparotomy of Perforation Peritonitis in 92 Years Old PatientSarah RonquilloNoch keine Bewertungen
- INSTRUCTIONS For The ADMINISTRATION of The MMSE-P and The CD 19117225744Document3 pagesINSTRUCTIONS For The ADMINISTRATION of The MMSE-P and The CD 19117225744Sarah RonquilloNoch keine Bewertungen
- APASL Consensus Guidelines On Invasive and Non Invasive Assessment of Hepatic Fibrosis A 2016 UpdateDocument30 pagesAPASL Consensus Guidelines On Invasive and Non Invasive Assessment of Hepatic Fibrosis A 2016 UpdateAdi Saputra100% (1)
- Geriatrics (Tra Intl)Document12 pagesGeriatrics (Tra Intl)Cess MarigondonNoch keine Bewertungen
- ThrombocytopeniaDocument12 pagesThrombocytopeniatantyNoch keine Bewertungen
- No Dokumen: Kkmoh-Ag2-Ak2 Arahan Kerja: Permohonan Peruntukan Penyelidikan KajianDocument26 pagesNo Dokumen: Kkmoh-Ag2-Ak2 Arahan Kerja: Permohonan Peruntukan Penyelidikan KajianneuroqehNoch keine Bewertungen
- Medication Study GuideDocument22 pagesMedication Study GuideArcenciel26100% (1)
- Antithrombotics PDFDocument14 pagesAntithrombotics PDFRizki Setiawan SultanNoch keine Bewertungen
- Preoperative Assessment. Plauntz (2007)Document17 pagesPreoperative Assessment. Plauntz (2007)Dario Cahuaza :VNoch keine Bewertungen
- Concise Manual of Cosmetic Dermatologic SurgeryDocument142 pagesConcise Manual of Cosmetic Dermatologic SurgerynzsargaziNoch keine Bewertungen
- Anaesthesia - 2024 - Mitchell - Principles For Management of Hip Fracture For Older Adults Taking Direct OralDocument11 pagesAnaesthesia - 2024 - Mitchell - Principles For Management of Hip Fracture For Older Adults Taking Direct Oralhelen.ashton5Noch keine Bewertungen
- Sustanon '250': Name of The MedicineDocument7 pagesSustanon '250': Name of The MedicineAmalia WardatulNoch keine Bewertungen
- Nclex PogiDocument8 pagesNclex Pogijackyd5Noch keine Bewertungen
- HNELHD CG 12 04 Warfarin Age Adjusted Dosing in AdultsDocument5 pagesHNELHD CG 12 04 Warfarin Age Adjusted Dosing in AdultsAnonymous 4txA8N8etNoch keine Bewertungen
- ABUHB - Clinical - 0780 AnticoagulationForHeartValveReplacementsMarch2019 PDFDocument9 pagesABUHB - Clinical - 0780 AnticoagulationForHeartValveReplacementsMarch2019 PDFErika KennedyNoch keine Bewertungen
- Fall 2021 Longitudinal Ippe SyllabusDocument7 pagesFall 2021 Longitudinal Ippe Syllabusapi-602288180Noch keine Bewertungen
- Anticoagulants, Direct and Indirect Thrombin InhibitorsDocument12 pagesAnticoagulants, Direct and Indirect Thrombin InhibitorsRinta Moon100% (1)
- High Alert MedicationsDocument1 pageHigh Alert MedicationspucukjayaNoch keine Bewertungen
- Ketorolac Tromethamine Injection Usp: Product MonographDocument41 pagesKetorolac Tromethamine Injection Usp: Product MonographWahyu AriawanNoch keine Bewertungen
- Atrial Fibrillation - Practice Essentials, Background, PathophysiologyDocument17 pagesAtrial Fibrillation - Practice Essentials, Background, PathophysiologyLorentina Den PanjaitanNoch keine Bewertungen
- Antiplatelet Therapy For The Secondary Prevention of Ischemic Stroke - UpToDateDocument13 pagesAntiplatelet Therapy For The Secondary Prevention of Ischemic Stroke - UpToDateSuci WijayaNoch keine Bewertungen
- SICH MGMTDocument12 pagesSICH MGMTLennon Ponta-oyNoch keine Bewertungen
- 2015-Journal of Thrombosis and Haemostasis PDFDocument997 pages2015-Journal of Thrombosis and Haemostasis PDFnikospapaioannouNoch keine Bewertungen
- Lecture 6 Pharma DR N AlhasaniDocument9 pagesLecture 6 Pharma DR N Alhasanialialahmedy24Noch keine Bewertungen
- SR Prabhu General Medicine For Dental PracticeDocument307 pagesSR Prabhu General Medicine For Dental PracticeNirmallya MukherjeeNoch keine Bewertungen
- Pulmonary EmbolismDocument20 pagesPulmonary Embolismdyah sekar ayuNoch keine Bewertungen
- Warren Jarboe - CV IptecDocument7 pagesWarren Jarboe - CV Iptecapi-610938913Noch keine Bewertungen
- Drug Study HeparinDocument2 pagesDrug Study HeparinArianne Nicole100% (1)
- 05-Pharmacology NCLEX ExcerptDocument14 pages05-Pharmacology NCLEX ExcerptShiraishiNoch keine Bewertungen
- Stroke Guidelines 20190724Document40 pagesStroke Guidelines 20190724Виктория МатяшNoch keine Bewertungen
- Atrial Fibrillation Occurring During Acute Hospitalization AHA 2023Document23 pagesAtrial Fibrillation Occurring During Acute Hospitalization AHA 2023Lena Hinojosa SarabiaNoch keine Bewertungen