Download as pdf or txt
You might also like
- Heart & Neck Vessel AssessmentDocument46 pagesHeart & Neck Vessel AssessmentLouise Nathalia VelasquezNoch keine Bewertungen
- NCP - AnemiaDocument7 pagesNCP - AnemiaJulian Ivaran Naceda90% (10)
- L3 Renal ClearanceDocument17 pagesL3 Renal ClearanceDeepa100% (2)
- PASOO Weight ManagementDocument4 pagesPASOO Weight ManagementNestor BalboaNoch keine Bewertungen
- Challacombe Scale Oral Dryness ENG PDFDocument1 pageChallacombe Scale Oral Dryness ENG PDFanimegawatiNoch keine Bewertungen
- Peptic UlcerDocument53 pagesPeptic UlcerHoney Lyn AlebioNoch keine Bewertungen
- Cardiomyopathy: Mrs. D. Melba Sahaya Sweety M.SC Nursing GimsarDocument55 pagesCardiomyopathy: Mrs. D. Melba Sahaya Sweety M.SC Nursing GimsarD. Melba S.S ChinnaNoch keine Bewertungen
- Hepatic Encephalopathy and ComaDocument19 pagesHepatic Encephalopathy and ComaJas Castro JoveroNoch keine Bewertungen
- Mental Health Nursing II NURS 2310: Unit 1 Basic Concepts of Mental Health and Mental IllnessDocument41 pagesMental Health Nursing II NURS 2310: Unit 1 Basic Concepts of Mental Health and Mental IllnessRocky Domingo LazaroNoch keine Bewertungen
- NCM 118 CARDIO LECTURE LIFE THREATENING EMERGENCY CONGESTIVE HEART FAILURE MVIMMACULATA 2021 For Canvas-1Document46 pagesNCM 118 CARDIO LECTURE LIFE THREATENING EMERGENCY CONGESTIVE HEART FAILURE MVIMMACULATA 2021 For Canvas-1Pollen Siega BunalNoch keine Bewertungen
- Respiratory Emergencies: Amy Bullock Amy - Bullock@students - Plymouth.ac - UkDocument34 pagesRespiratory Emergencies: Amy Bullock Amy - Bullock@students - Plymouth.ac - UkThea BerteaNoch keine Bewertungen
- Management For CTD - MsDocument63 pagesManagement For CTD - MsNarz CupahanNoch keine Bewertungen
- Chapter 48 - Skin Integrity and Wound CareDocument13 pagesChapter 48 - Skin Integrity and Wound CareHaji Raji100% (1)
- Acute Biologic CrisisDocument106 pagesAcute Biologic CrisisLisette Grace Umadhay CabalangNoch keine Bewertungen
- Myocardial InfarctionDocument3 pagesMyocardial Infarctionaja_delNoch keine Bewertungen
- Test Bank For Psychiatric Mental Health Nursing 1st Edition by PotterDocument38 pagesTest Bank For Psychiatric Mental Health Nursing 1st Edition by Potterlionelhuynhg7cNoch keine Bewertungen
- Acute Myocardial InfarctionDocument22 pagesAcute Myocardial InfarctionkpsuanNoch keine Bewertungen
- NCM118 Lecture 1Document18 pagesNCM118 Lecture 1mirai desuNoch keine Bewertungen
- Lesson 3 Hemodynamic Monitoring Semi Finals 3Document18 pagesLesson 3 Hemodynamic Monitoring Semi Finals 3Juffer ConconNoch keine Bewertungen
- Biologic Crisis: Prepared By: Ronnie M. Amazona, RN, ManDocument162 pagesBiologic Crisis: Prepared By: Ronnie M. Amazona, RN, ManLex CatNoch keine Bewertungen
- Scope of Nle910Document254 pagesScope of Nle910ericNoch keine Bewertungen
- Digestive Q3Document22 pagesDigestive Q3Geevee Naganag VentulaNoch keine Bewertungen
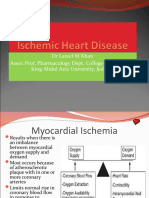
- Ischemic Heart Disease Revised LMKDocument50 pagesIschemic Heart Disease Revised LMKLateef KhanNoch keine Bewertungen
- IVT ComplicationsDocument6 pagesIVT ComplicationsMercicae ANoch keine Bewertungen
- Acute Biologic Crisis 1Document45 pagesAcute Biologic Crisis 1Nina OaipNoch keine Bewertungen
- PANCREATITISDocument38 pagesPANCREATITISVEDHIKAVIJAYANNoch keine Bewertungen
- Anatomy of The Heart: Materials Pre-Lab QuizDocument14 pagesAnatomy of The Heart: Materials Pre-Lab QuizAnonymous dRAu54Noch keine Bewertungen
- High Acuity and Emergency SituationDocument9 pagesHigh Acuity and Emergency SituationRENEROSE TORRESNoch keine Bewertungen
- 780 Adult Cardio Resp Assess DSTDocument10 pages780 Adult Cardio Resp Assess DSTGursangeet Kaur100% (1)
- Lower Airway DiseasesDocument70 pagesLower Airway DiseasesAavash PradhanNoch keine Bewertungen
- Midterm Reviewer Med Surg LecDocument28 pagesMidterm Reviewer Med Surg LecSammNoch keine Bewertungen
- Cardio 1Document13 pagesCardio 1TinNoch keine Bewertungen
- Maternal and Child NursingDocument13 pagesMaternal and Child NursingCarrel Relojero CarlosNoch keine Bewertungen
- Sirs ModsDocument10 pagesSirs ModsRENEROSE TORRESNoch keine Bewertungen
- ECG Study GuideDocument7 pagesECG Study GuideannaNoch keine Bewertungen
- Management of ArrhythmiasDocument4 pagesManagement of ArrhythmiasAray Al-AfiqahNoch keine Bewertungen
- Pneumothorax-WPS OfficeDocument18 pagesPneumothorax-WPS Officelea jumawanNoch keine Bewertungen
- Respiratory SystemDocument35 pagesRespiratory SystemPatricia Mae SalazarNoch keine Bewertungen
- Ethical Principles: Example: Surgery, or Any ProcedureDocument3 pagesEthical Principles: Example: Surgery, or Any ProcedureKevin Miguel Rivera100% (1)
- PneumoniasDocument58 pagesPneumoniasKai Edmond MarvellaNoch keine Bewertungen
- September 13 - NCM 112 (Mam G)Document2 pagesSeptember 13 - NCM 112 (Mam G)Aaron DayloNoch keine Bewertungen
- Nursing Care of Clients With Cardiovascular DisorderDocument16 pagesNursing Care of Clients With Cardiovascular DisorderLuna MarieNoch keine Bewertungen
- Renal EmergenciesDocument8 pagesRenal EmergenciesRENEROSE TORRESNoch keine Bewertungen
- NCMB314 Prelim ReadingsDocument77 pagesNCMB314 Prelim ReadingsNine SoleilNoch keine Bewertungen
- Cardiology Medsurg LectureDocument9 pagesCardiology Medsurg LectureTine GuibaoNoch keine Bewertungen
- Cardio NursingDocument141 pagesCardio NursingKhatlen BagaresNoch keine Bewertungen
- Disorder of Respiratory SystemDocument89 pagesDisorder of Respiratory SystemDarine Nasr100% (1)
- Perioperative NursingDocument88 pagesPerioperative Nursingdaljit chahalNoch keine Bewertungen
- NUR100 Sherpath Skin Overview + Skin IntegrityDocument15 pagesNUR100 Sherpath Skin Overview + Skin Integritycaloy2345caloy100% (1)
- Diarrhea: Persistent If 2-4 Weeks, and Chronic If 4 Weeks in DurationDocument12 pagesDiarrhea: Persistent If 2-4 Weeks, and Chronic If 4 Weeks in DurationAnonymous IWRTYznDZnNoch keine Bewertungen
- Nursing RLEDocument19 pagesNursing RLEPatricia AdiaoNoch keine Bewertungen
- Post Operative HemorrhageDocument16 pagesPost Operative Hemorrhagenishimura89Noch keine Bewertungen
- (NLE) ColostomyDocument1 page(NLE) Colostomyparisfrance89Noch keine Bewertungen
- SuctioningDocument30 pagesSuctioningbajaoc60% (5)
- Respiratory Emx ARF ARDSDocument12 pagesRespiratory Emx ARF ARDSRENEROSE TORRESNoch keine Bewertungen
- MINI CP Angina PectorisDocument11 pagesMINI CP Angina Pectorisyasira100% (1)
- Nursing Care of The Client With High-Risk Labor and DeliveryDocument23 pagesNursing Care of The Client With High-Risk Labor and DeliveryMarie Ashley CasiaNoch keine Bewertungen
- Neurologic NCLEX Practice Test Part 1Document6 pagesNeurologic NCLEX Practice Test Part 1ojoj2206Noch keine Bewertungen
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNoch keine Bewertungen
- Leaping the Hurdles: The Essential Companion Guide for International Medical Graduates on their Australian JourneyFrom EverandLeaping the Hurdles: The Essential Companion Guide for International Medical Graduates on their Australian JourneyNoch keine Bewertungen
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- NURSING EMERGENCIES. 10 BASED TEST QUESTIONS WITH BIBLIOGRAPHYFrom EverandNURSING EMERGENCIES. 10 BASED TEST QUESTIONS WITH BIBLIOGRAPHYNoch keine Bewertungen
- CA - Adult Health Nursing PDFDocument55 pagesCA - Adult Health Nursing PDFMarvin Heramis RyanNoch keine Bewertungen
- Divine Intervention Step 2CK Podcasts Notes - Read Only File - Docx (Dragged) 4Document3 pagesDivine Intervention Step 2CK Podcasts Notes - Read Only File - Docx (Dragged) 4winston1234Noch keine Bewertungen
- S1 GEN. CHEM 11 Q2 Performance Task (Part I) Abstract G4Document3 pagesS1 GEN. CHEM 11 Q2 Performance Task (Part I) Abstract G4Kai SamaNoch keine Bewertungen
- Oral Comm Quiz 2Document1 pageOral Comm Quiz 2Kai SamaNoch keine Bewertungen
- Grade 11 ReviewerDocument2 pagesGrade 11 ReviewerKai SamaNoch keine Bewertungen
- NCM 118 MIDTERMS PG 7Document1 pageNCM 118 MIDTERMS PG 7Kai SamaNoch keine Bewertungen
- Em-Tech ReviewerDocument2 pagesEm-Tech ReviewerKai SamaNoch keine Bewertungen
- Em-Tech ReviewerDocument3 pagesEm-Tech ReviewerKai SamaNoch keine Bewertungen
- COVID-19 Detection by RT-PCR.: Page 1 of 2Document2 pagesCOVID-19 Detection by RT-PCR.: Page 1 of 2Basheer Thalangara MamooNoch keine Bewertungen
- Diabetes in PregnancyDocument11 pagesDiabetes in PregnancyAlana CaballeroNoch keine Bewertungen
- ayur-MED 1Document34 pagesayur-MED 1Narasannapeta PatanjaliNoch keine Bewertungen
- Handbook For Principles and Practice of Gynecologic Oncology-1Document379 pagesHandbook For Principles and Practice of Gynecologic Oncology-1shiv100% (1)
- Jurnal Hasil Penelitian Kimed Antikanker Kelompok 7Document11 pagesJurnal Hasil Penelitian Kimed Antikanker Kelompok 7PerawNoch keine Bewertungen
- Homeopathic Remedies For Hydronephrosis - Homeo ExpertDocument7 pagesHomeopathic Remedies For Hydronephrosis - Homeo ExpertDr. Kazy Habibur RahmanNoch keine Bewertungen
- Morgan Mikhails Clinical Anesthesiology 6th Ed 2018 (2114-2211)Document98 pagesMorgan Mikhails Clinical Anesthesiology 6th Ed 2018 (2114-2211)Wiwik SundariNoch keine Bewertungen
- Parreno, Jonar Valler 1981024627Document1 pageParreno, Jonar Valler 1981024627charlies parrenoNoch keine Bewertungen
- Nuclear Medicine Technician or MedicalDocument2 pagesNuclear Medicine Technician or Medicalapi-79207760Noch keine Bewertungen
- MyChart - Test Details PDFDocument3 pagesMyChart - Test Details PDFAnonymous iy0yzUJOOrNoch keine Bewertungen
- Medicine 018 Final PDFDocument22 pagesMedicine 018 Final PDFdrkefyalewtayeNoch keine Bewertungen
- Pengaruh Pijat Bayi Terhadap Kelancaran Bab Pada Balita Usia 12-24 BulanDocument6 pagesPengaruh Pijat Bayi Terhadap Kelancaran Bab Pada Balita Usia 12-24 BulanAna SafitriNoch keine Bewertungen
- 01 Avian Inflam PDFDocument13 pages01 Avian Inflam PDFDrPraveen DodwaNoch keine Bewertungen
- A-Z Family Medical EncyclopediaDocument815 pagesA-Z Family Medical Encyclopediasunilas218408100% (10)
- Ophthalmologic Approach To Chemical Burns - Background, Pathophysiology, EpidemiologyDocument6 pagesOphthalmologic Approach To Chemical Burns - Background, Pathophysiology, EpidemiologyAnonymous S0MyRHNoch keine Bewertungen
- Clinical Case of A Patient With Aortic Periprosthetic InfectionDocument4 pagesClinical Case of A Patient With Aortic Periprosthetic InfectionAthenaeum Scientific PublishersNoch keine Bewertungen
- Smith Lemli Optiz Syndrome Group 7Document10 pagesSmith Lemli Optiz Syndrome Group 7EULA MARIE JOVERNoch keine Bewertungen
- Wa0011.Document17 pagesWa0011.Aakash SpNoch keine Bewertungen
- Acute Interstitial Nephritis 2Document19 pagesAcute Interstitial Nephritis 2Paul SinsNoch keine Bewertungen
- What Is MagnetotherapyDocument2 pagesWhat Is MagnetotherapyMagic LifeNoch keine Bewertungen
- Nupc 113 Module IDocument110 pagesNupc 113 Module IAthena PasabingNoch keine Bewertungen
- Entry Level PharmD Program PDFDocument2 pagesEntry Level PharmD Program PDFDavid HosamNoch keine Bewertungen
- Dolor CVNADocument15 pagesDolor CVNAStephania MendozaNoch keine Bewertungen
- Análise Temporal e Comparativa Entre Métodos de Dissecção Do Abdômen para Exposição Aorto-CavalDocument4 pagesAnálise Temporal e Comparativa Entre Métodos de Dissecção Do Abdômen para Exposição Aorto-CavalariellafisioterapeutaNoch keine Bewertungen
- Introduction To Clinical and Counselling Psychology 08 - Interventions - The FoundationsDocument35 pagesIntroduction To Clinical and Counselling Psychology 08 - Interventions - The FoundationsRam LifschitzNoch keine Bewertungen
- What Is An EEG Used For?Document1 pageWhat Is An EEG Used For?Abdullah Bin YahyaNoch keine Bewertungen