Download as pdf or txt
You might also like
- Full Download Test Bank For Health Economics and Policy 7th Edition Henderson PDF Full ChapterDocument34 pagesFull Download Test Bank For Health Economics and Policy 7th Edition Henderson PDF Full Chapterjakraging7odbt95% (20)
- Mental and Emotional Health PowerpointDocument36 pagesMental and Emotional Health PowerpointYen Aduana90% (10)
- Parental Capability Assssment Report (For Child - )Document5 pagesParental Capability Assssment Report (For Child - )APRIL ANNE BALASON AGSOLID100% (4)
- The Future Immigration Consultants Service AgreementDocument9 pagesThe Future Immigration Consultants Service AgreementKazandra Cassidy GarciaNoch keine Bewertungen
- Mobis Isir ManualDocument17 pagesMobis Isir ManualGabriel MolinaNoch keine Bewertungen
- 4gwifi User ManualDocument16 pages4gwifi User ManualYugandhar YuguNoch keine Bewertungen
- NEFT/RTGS E-Receipt: Dayananda Sagar Academy of Tech and MGMT ICL9080754472685 ICIC0000103Document3 pagesNEFT/RTGS E-Receipt: Dayananda Sagar Academy of Tech and MGMT ICL9080754472685 ICIC0000103study materialNoch keine Bewertungen
- Department of Medicine Report 2019Document49 pagesDepartment of Medicine Report 2019Taylor LaframboiseNoch keine Bewertungen
- Resilience360 Annual Risk Report 2018Document45 pagesResilience360 Annual Risk Report 2018M QasimNoch keine Bewertungen
- Arwind Thakare - Client Services Technician - CY9Document3 pagesArwind Thakare - Client Services Technician - CY9Chaitanya GhanokarNoch keine Bewertungen
- Assignment 2Document8 pagesAssignment 2Kumaran ViswanathanNoch keine Bewertungen
- AEI-FPD 47 - Pre-Joining Declaration For TraineesDocument2 pagesAEI-FPD 47 - Pre-Joining Declaration For TraineesKuldeep KumarNoch keine Bewertungen
- 2012 Niperjee Meritlist GenDocument21 pages2012 Niperjee Meritlist GenSiri Kalyan100% (1)
- CMDC Construction Management in Developing Countries Chapter 1 July2023Document78 pagesCMDC Construction Management in Developing Countries Chapter 1 July2023harikshresthaNoch keine Bewertungen
- Final Report To The People 2016 2021 PRRDDocument270 pagesFinal Report To The People 2016 2021 PRRDJustine KimNoch keine Bewertungen
- Process For Registration of Password Based User On SPEED-e FacilityDocument14 pagesProcess For Registration of Password Based User On SPEED-e FacilitySathishNoch keine Bewertungen
- Challan AxisDocument3 pagesChallan AxisSumit Darak50% (2)
- 2022 05 11 Russian ADR+GDRsDocument1 page2022 05 11 Russian ADR+GDRsSouthey CapitalNoch keine Bewertungen
- Pre Bid Conference and ClarificationsDocument5 pagesPre Bid Conference and ClarificationsNeighborof AbhinandanindiaNoch keine Bewertungen
- GM Cruise ProbeDocument2 pagesGM Cruise ProbeJoey KlenderNoch keine Bewertungen
- Fast Food Competition-3-29Document27 pagesFast Food Competition-3-29Thanh Hà TrầnNoch keine Bewertungen
- LawsuitDocument53 pagesLawsuitGizmodo EditNoch keine Bewertungen
- Taitz, Hale Complaint 05 04 2009Document85 pagesTaitz, Hale Complaint 05 04 2009haneno100% (11)
- 4-Job Application Form For The Post of LHVDocument2 pages4-Job Application Form For The Post of LHVHajveri Photo State Sambrial100% (1)
- POLS151 Midterm 5Document5 pagesPOLS151 Midterm 5Sean Anjenette GalvanteNoch keine Bewertungen
- Advance Panel (Panel) Bharti RealtyDocument2 pagesAdvance Panel (Panel) Bharti Realtyanon-435756100% (3)
- OLX - Software Requirement Specification SRS: Software Engineering (Lovely Professional University)Document7 pagesOLX - Software Requirement Specification SRS: Software Engineering (Lovely Professional University)Sai Swaroop0% (1)
- Sinclair 2023 Physician Verification FormDocument1 pageSinclair 2023 Physician Verification FormMaritza NunezNoch keine Bewertungen
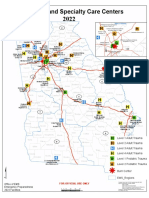
- Georgia's Designated Trauma and Specialty Care CentersDocument1 pageGeorgia's Designated Trauma and Specialty Care CentersLindsey BasyeNoch keine Bewertungen
- CV MinhHieuDocument2 pagesCV MinhHieuHiếu Trần Lê MinhNoch keine Bewertungen
- Mertoglu and Gunay 2017Document5 pagesMertoglu and Gunay 2017Via MeysaNoch keine Bewertungen
- Final Comprehensive Case Study - Noday!Document11 pagesFinal Comprehensive Case Study - Noday!natalie nodayNoch keine Bewertungen
- SRF-Serviced Plots-Manual Submission ONLYDocument1 pageSRF-Serviced Plots-Manual Submission ONLYARUL SANKARANNoch keine Bewertungen
- In SHORT March 2021 7rgij5Document59 pagesIn SHORT March 2021 7rgij5Mayur BNoch keine Bewertungen
- Wi Resume-ApplicationDocument2 pagesWi Resume-ApplicationRichverr LovelyNoch keine Bewertungen
- Creative Project FinalDocument7 pagesCreative Project Finalapi-654504494Noch keine Bewertungen
- Autoclave ManualDocument60 pagesAutoclave ManualDiệp Long HồNoch keine Bewertungen
- Marathon NotesDocument341 pagesMarathon NotesLokesh Agarwalla100% (1)
- ACFrOgACirloeIgwRSPxDsVrqnW ykcf1H-Pj9oMMLoG7Ttuox0JRVfH1eHjjYD0RYenQhep8VHm11Lz36fGpnqNS 7zG5a423VSibufOBi3d9U4VE3Bly9y5hxp3Zo PDFDocument4 pagesACFrOgACirloeIgwRSPxDsVrqnW ykcf1H-Pj9oMMLoG7Ttuox0JRVfH1eHjjYD0RYenQhep8VHm11Lz36fGpnqNS 7zG5a423VSibufOBi3d9U4VE3Bly9y5hxp3Zo PDFRichard MenthNoch keine Bewertungen
- Falaknuma Exp Sleeper Class (SL)Document2 pagesFalaknuma Exp Sleeper Class (SL)G DalirajuNoch keine Bewertungen
- Ao 2012 0001Document56 pagesAo 2012 0001Dennis FuentesNoch keine Bewertungen
- P V Fix Higgins Molitor Null and Null Decision and Order Granting The Peoples Motions To Consolidate and Co Conspirator Statements 02-15-23Document7 pagesP V Fix Higgins Molitor Null and Null Decision and Order Granting The Peoples Motions To Consolidate and Co Conspirator Statements 02-15-23Fergus BurnsNoch keine Bewertungen
- Emirates and The UK: MillionDocument2 pagesEmirates and The UK: MillionMinh PhượngNoch keine Bewertungen
- STP Analysis of AirtelDocument5 pagesSTP Analysis of AirtelSahil VaishyaNoch keine Bewertungen
- Proposed Learning ModulesDocument9 pagesProposed Learning Modulesapi-664608528Noch keine Bewertungen
- FILM330 Problems 2Document5 pagesFILM330 Problems 2Raisya febiyaneeeNoch keine Bewertungen
- Aishwarya Viva - PPT ProjectDocument71 pagesAishwarya Viva - PPT Projectaishwarya damleNoch keine Bewertungen
- Loveless AppealDocument4 pagesLoveless AppealNevin SmithNoch keine Bewertungen
- ERB-2023-232 CAS Golosino ProposalDocument61 pagesERB-2023-232 CAS Golosino Proposalanthonymatthew.nemenzoNoch keine Bewertungen
- Loan Application FormDocument5 pagesLoan Application FormSamantha SinghNoch keine Bewertungen
- Pestel Analysis FurnitureDocument4 pagesPestel Analysis FurnituregraceNoch keine Bewertungen
- Personal Development ReviewerDocument5 pagesPersonal Development ReviewerTrixie Ann AldayNoch keine Bewertungen
- Tac Doc 01 2 Issue 2 Rev 0 Information Package Latest As Registered With TecsDocument17 pagesTac Doc 01 2 Issue 2 Rev 0 Information Package Latest As Registered With TecsWildan Amar ZainNoch keine Bewertungen
- Key Information Sheet: IhealthDocument18 pagesKey Information Sheet: Ihealthmksnake77Noch keine Bewertungen
- Mitchell Board of Education Agenda Oct. 11Document50 pagesMitchell Board of Education Agenda Oct. 11inforumdocsNoch keine Bewertungen
- Covid19 HypercoagulabilityDocument22 pagesCovid19 Hypercoagulability陳瑞豐Noch keine Bewertungen
- Virtusa Jatayu Season 3 Student GuideDocument1 pageVirtusa Jatayu Season 3 Student GuideSai UthejNoch keine Bewertungen
- Uqullox4 Qti20221027Document2 pagesUqullox4 Qti20221027Khawar Riaz100% (1)
- Nursing Home Vaccine Order 1-19-22Document3 pagesNursing Home Vaccine Order 1-19-22WXYZ-TV Channel 7 DetroitNoch keine Bewertungen
- Filed Lopez Moran Complaint 2023-04-11Document25 pagesFiled Lopez Moran Complaint 2023-04-11LehighValley NewsdotcomNoch keine Bewertungen
- Alico Indemnity Medical Claim FormDocument2 pagesAlico Indemnity Medical Claim FormJalal Al-QutobNoch keine Bewertungen
- Accidental Injury Claim Form: Policy NumberDocument2 pagesAccidental Injury Claim Form: Policy NumberMary MurphyNoch keine Bewertungen
- Continuing Disability Claim FormDocument3 pagesContinuing Disability Claim FormAndrea DunnavilleNoch keine Bewertungen
- How To Reduce PollutionDocument3 pagesHow To Reduce Pollutionalyaa_haziraNoch keine Bewertungen
- Hope ReviewerDocument4 pagesHope ReviewerJade ivan parrochaNoch keine Bewertungen
- The Chemistry of L-Ascorbic Acid Derivatives PDFDocument245 pagesThe Chemistry of L-Ascorbic Acid Derivatives PDFnonameNoch keine Bewertungen
- PHAR0424Document2 pagesPHAR0424Rappler0% (1)
- The Healing Practice of Pagtatawas Among Pangasinense Traditional HealersDocument2 pagesThe Healing Practice of Pagtatawas Among Pangasinense Traditional HealersChristine VelasquezNoch keine Bewertungen
- Visitor Counter Based On TemperatureDocument17 pagesVisitor Counter Based On TemperatureCnp1 Cnp1Noch keine Bewertungen
- CTGDocument242 pagesCTGKishore Kumar RaviChandranNoch keine Bewertungen
- Conversion Table For PressureDocument4 pagesConversion Table For Pressuredassi99Noch keine Bewertungen
- Capgemini 1Document27 pagesCapgemini 1Paavni SharmaNoch keine Bewertungen
- Enteb UnilabDocument4 pagesEnteb UnilabKyla Isidro0% (1)
- Cas Path Fit1 Study Guide 2021Document72 pagesCas Path Fit1 Study Guide 2021Martha Therese CapinNoch keine Bewertungen
- 2 Dimentions of NSTPDocument22 pages2 Dimentions of NSTPkurou hazamaNoch keine Bewertungen
- Boys On The Move English - Facilitator BookDocument52 pagesBoys On The Move English - Facilitator BookslezinaNoch keine Bewertungen
- Upscaling Fight Against Illiict Brew Reporting ToolDocument3 pagesUpscaling Fight Against Illiict Brew Reporting Tooldragon labNoch keine Bewertungen
- HTD 2008Document208 pagesHTD 2008mikewat20Noch keine Bewertungen
- Ijcdc: Comparative Efficacy of Tea Tree Oil Nanoemulgel and Tea Tree Oil Gel Against Candida AlbicansDocument6 pagesIjcdc: Comparative Efficacy of Tea Tree Oil Nanoemulgel and Tea Tree Oil Gel Against Candida Albicansal rzNoch keine Bewertungen
- Law and Med - 2Document9 pagesLaw and Med - 2Anirudh RanaNoch keine Bewertungen
- 802.034 Datasheet Phyaction CL v1.5 en LRDocument4 pages802.034 Datasheet Phyaction CL v1.5 en LRSofie BeckersNoch keine Bewertungen
- Pre Employment Medical Declaration Form - 2022Document2 pagesPre Employment Medical Declaration Form - 2022Neel GhoshNoch keine Bewertungen
- Hernia Inguinal - ShouldiceDocument25 pagesHernia Inguinal - ShouldiceBrunoRochNoch keine Bewertungen
- Indeks Dokter 2020Document311 pagesIndeks Dokter 2020rekam medisNoch keine Bewertungen
- Reading Exam Anti Smoking Law. PAU-ORIENTED 2º BachilleratoDocument1 pageReading Exam Anti Smoking Law. PAU-ORIENTED 2º Bachilleratoteresa guerreroNoch keine Bewertungen
- Mental HealthDocument18 pagesMental HealthAnshika SrivastavaNoch keine Bewertungen
- Analytical Method Validation Used in CleaningDocument46 pagesAnalytical Method Validation Used in Cleaningkavya nainitaNoch keine Bewertungen
- Unit 7 INTERESTS - HOBBIESDocument2 pagesUnit 7 INTERESTS - HOBBIESThanh VẹnNoch keine Bewertungen
- Product Catalog 2023Document54 pagesProduct Catalog 2023sdvfsNoch keine Bewertungen
- Nursing Care Plan - FatigueDocument2 pagesNursing Care Plan - FatigueDaniel Andre S. SomorayNoch keine Bewertungen